Melanoma Institute Australia, University of Sydney, Sydney, New South Wales, Australia.
Department of Dermatology, Leiden University Medical Centre, Leiden, the Netherlands.
Br J Surg. 2019 Sep;106(10):1319-1326. doi: 10.1002/bjs.11262. Epub 2019 Jul 16.
Identifying patients with sentinel node-negative melanoma at high risk of recurrence or death is important. The European Organisation for Research and Treatment of Cancer (EORTC) recently developed a prognostic model including Breslow thickness, ulceration and site of the primary tumour. The aims of the present study were to validate this prognostic model externally and to assess whether it could be improved by adding other prognostic factors.
Patients with sentinel node-negative cutaneous melanoma were included in this retrospective single-institution study. The β values of the EORTC prognostic model were used to predict recurrence-free survival and melanoma-specific survival. The predictive performance was assessed by discrimination (c-index) and calibration. Seeking to improve the performance of the model, additional variables were added to a Cox proportional hazards model.
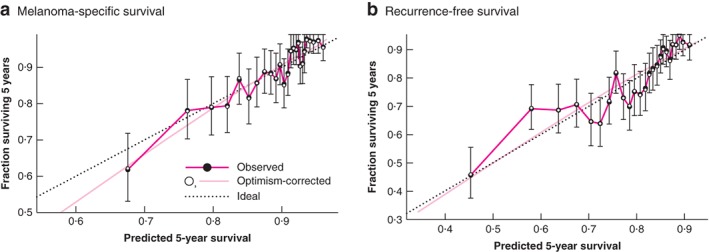
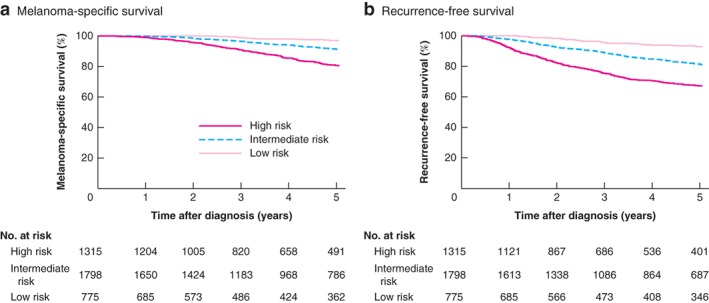
Some 4235 patients with sentinel node-negative cutaneous melanoma were included. The median follow-up time was 50 (i.q.r. 18·5-81·5) months. Recurrences and deaths from melanoma numbered 793 (18·7 per cent) and 456 (10·8 per cent) respectively. Validation of the EORTC model showed good calibration for both outcomes, and a c-index of 0·69. The c-index was only marginally improved to 0·71 when other significant prognostic factors (sex, age, tumour type, mitotic rate) were added.
This study validated the EORTC prognostic model for recurrence-free and melanoma-specific survival of patients with negative sentinel nodes. The addition of other prognostic factors only improved the model marginally. The validated EORTC model could be used for personalizing follow-up and selecting high-risk patients for trials of adjuvant systemic therapy.
识别无前哨淋巴结转移黑色素瘤且具有高复发或死亡风险的患者非常重要。欧洲癌症研究与治疗组织(EORTC)最近开发了一种预后模型,包括 Breslow 厚度、溃疡和原发肿瘤部位。本研究旨在对该预后模型进行外部验证,并评估是否可以通过添加其他预后因素来进行改进。
本回顾性单中心研究纳入了无前哨淋巴结转移的皮肤黑色素瘤患者。使用 EORTC 预后模型的β值预测无复发生存率和黑色素瘤特异性生存率。通过判别(c 指数)和校准评估预测性能。为了提高模型的性能,向 Cox 比例风险模型中添加了其他变量。
共纳入 4235 例无前哨淋巴结转移的皮肤黑色素瘤患者。中位随访时间为 50(IQR 18.5-81.5)个月。分别有 793 例(18.7%)和 456 例(10.8%)患者发生复发和死于黑色素瘤。EORTC 模型的验证结果显示,两种结局的校准均较好,c 指数为 0.69。当加入其他显著的预后因素(性别、年龄、肿瘤类型、有丝分裂率)后,c 指数仅略有提高至 0.71。
本研究验证了 EORTC 模型在预测无前哨淋巴结转移黑色素瘤患者的无复发生存率和黑色素瘤特异性生存率方面的有效性。添加其他预后因素仅略微改善了模型。验证后的 EORTC 模型可用于个性化随访,并选择高危患者进行辅助系统性治疗的临床试验。