Ekulu Pepe M, Nkoy Agathe B, Betukumesu Dieumerci K, Aloni Michel N, Makulo Jean Robert R, Sumaili Ernest K, Mafuta Eric M, Elmonem Mohamed A, Arcolino Fanny O, Kitetele Faustin N, Lepira François B, van den Heuvel Lambertus P, Levtchenko Elena N
Department of Development and Regeneration, KU Leuven, Leuven, Belgium.
Division of Nephrology, Department of Pediatrics, University Hospital of Kinshasa, Faculty of Medicine, University of Kinshasa, Kinshasa, Democratic Republic of Congo.
Kidney Int Rep. 2019 Apr 11;4(7):930-938. doi: 10.1016/j.ekir.2019.04.002. eCollection 2019 Jul.
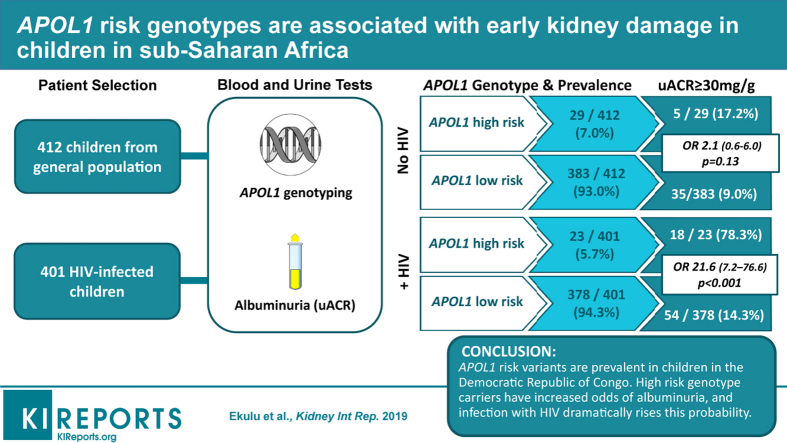
Apolipoprotein-L1 () risk variants G1 and G2 increase the risk of chronic kidney disease (CKD), including HIV-related CKD, among African Americans. However, such data from populations living in Africa, especially children, remain limited. Our research aimed to determine the prevalence of risk variants and to assess the association between these variants and early-stage CKD in the general pediatric population and HIV-infected children.
In a cross-sectional study, we enrolled 412 children from the general population and 401 HIV-infected children in Kinshasa, Democratic Republic of Congo (DRC). high-risk genotype (HRG) was defined by the presence of 2 risk variants (G1/G1, G2/G2, or G1/G2), and low-risk genotype (LRG) by the presence of 0 or 1 risk variants. The main outcome was elevated albuminuria, defined as a urinary albumin/creatinine ratio ≥30 mg/g.
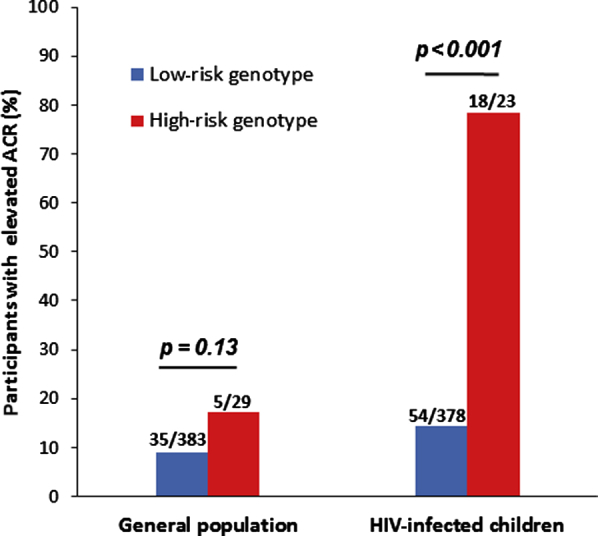
sequence analysis revealed that in the general population, 29 of 412 participants (7.0%) carried HRG, 84 of 412 (20.4%) carried the G1/G0 genotype, and 61 of 412 (14.8%) carried the G2/G0 genotype. In HIV-infected children, 23 of 401 (5.7%) carried HRG, and the same trend as in the general population was observed in regard to the prevalence of LRG. Univariate analysis showed that in the general population, 5 of 29 participants (17.2%) carrying HRG had elevated albuminuria, compared with 35 of 383 (9.0%) with LRG (odds ratio [OR] 2.1, 95% confidence interval [CI] 0.6-6.0; = 0.13). In HIV-infected children, participants who carried APOL1 HRG had almost 22-fold increased odds of albuminuria compared to those with LRG.
The risk variants are prevalent in children living in DRC. HRG carriers have increased odds of early kidney disease, and infection with HIV dramatically increases this probability.
载脂蛋白L1(APOL1)风险变异体G1和G2会增加非裔美国人患慢性肾脏病(CKD)的风险,包括与HIV相关的CKD。然而,来自非洲人群,尤其是儿童的此类数据仍然有限。我们的研究旨在确定APOL1风险变异体的患病率,并评估这些变异体与普通儿科人群和HIV感染儿童早期CKD之间的关联。
在一项横断面研究中,我们纳入了刚果民主共和国(DRC)金沙萨的412名普通儿童和401名HIV感染儿童。高风险基因型(HRG)定义为存在2个风险变异体(G1/G1、G2/G2或G1/G2),低风险基因型(LRG)定义为存在0个或1个风险变异体。主要结局是蛋白尿升高,定义为尿白蛋白/肌酐比值≥30mg/g。
序列分析显示,在普通人群中,412名参与者中有29名(7.0%)携带HRG,412名中有84名(20.4%)携带G1/G0基因型,412名中有61名(14.8%)携带G2/G0基因型。在HIV感染儿童中,401名中有23名(5.7%)携带HRG,LRG患病率与普通人群观察到的趋势相同。单因素分析显示,在普通人群中,29名携带HRG的参与者中有5名(17.2%)蛋白尿升高,而383名携带LRG的参与者中有35名(9.0%)蛋白尿升高(比值比[OR]2.1,95%置信区间[CI]0.6 - 6.0;P = 0.13)。在HIV感染儿童中,携带APOL1 HRG的参与者蛋白尿的几率比携带LRG的参与者几乎高22倍。
APOL1风险变异体在生活在DRC的儿童中普遍存在。HRG携带者患早期肾病的几率增加,而HIV感染会显著增加这种可能性。