Department of Surgery and Transplant Center, University Hospital Martin and Jessenius Medical Faculty, Comenius University, Kollárova 2, Martin, 036 01, Slovak Republic.
Ist Department of Internal Diseases, University Hospital Martin and Jessenius Medical Faculty, Comenius University Kollárova 2, Martin, 036 01, Slovak Republic.
BMC Nephrol. 2019 Jul 18;20(1):272. doi: 10.1186/s12882-019-1449-0.
Acute kidney injury (AKI) affects approximately 13% of patients undergoing major abdominal surgery, and is a common and important clinical sign of perioperative injury. The aim of our analysis was to identify risk factors for AKI in elderly patients with no known kidney disease at the time of surgery, and to evaluate their 30-day, 12-month and 5-year survival.
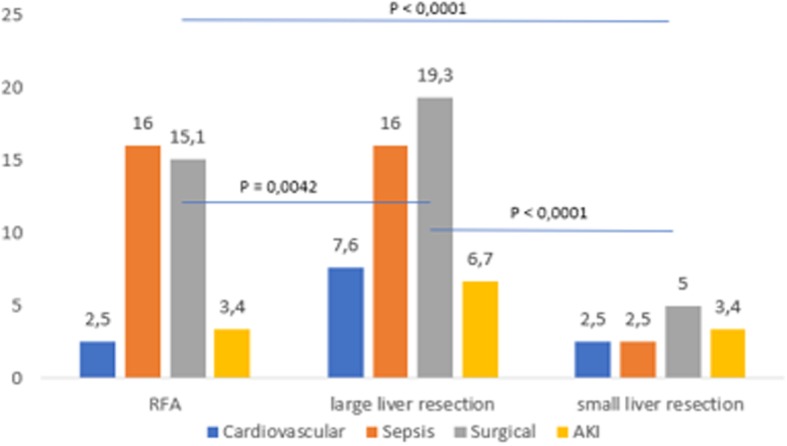
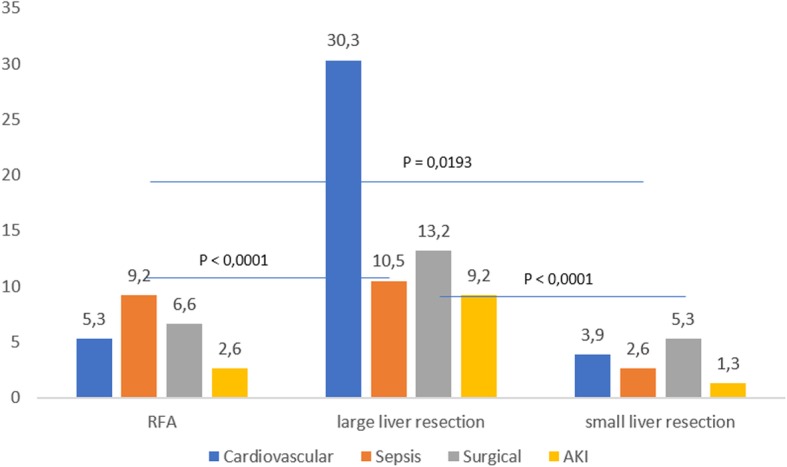
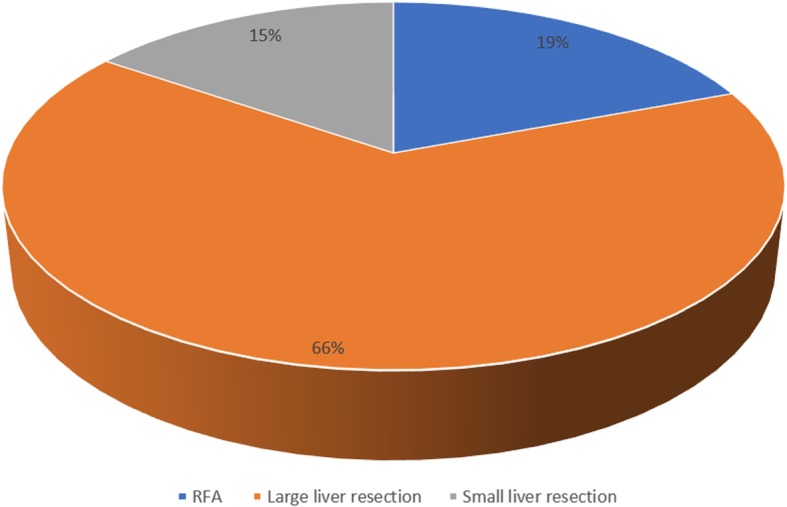
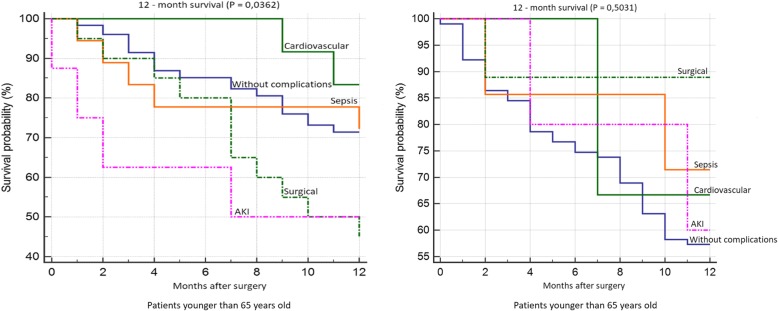
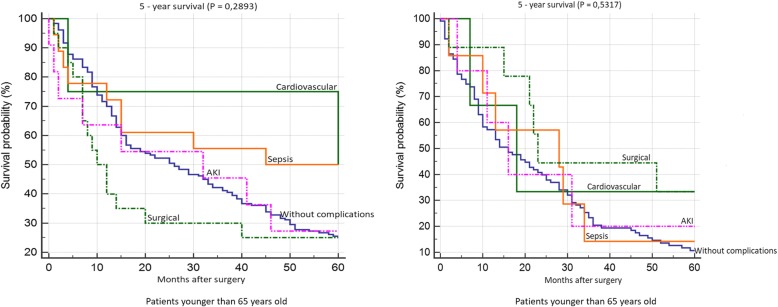
We performed a retrospective analysis on a group of 785 patients after liver resection to determine the incidence of complications (AKI - according to KDIGO classification, sepsis, cardiovascular and surgical complications). All patients had normal kidney function prior to surgery. We determined risk factors for the development of AKI for two groups of patients, stratified for age: patients younger than 65 years, and patients older than 65 years.
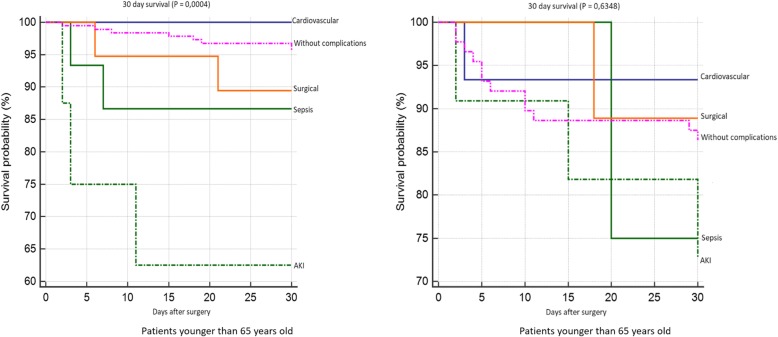
The incidence of complications was significantly higher in the group of patients older than 65 years (n = 76) than in younger patients (n = 119) (P = 0.0496). In the group of younger patients, significantly worse 30-day survival was observed for patients who developed AKI (P = 0.0004). We identified the following independent risk factors for AKI: male gender (HR 10,3834; P = 0,0238), histological identification of colorectal carcinoma metastases (HR 2,8651; P = 0,0499), surgery duration longer than 300 min (HR 6,0096; P < 0,0001), blood loss of more than 500 ml (HR 10,5857; P = 0,0012), and the need for more than 500 ml of fresh frozen plasma during surgery ml (HR 2,4878; P < 0,0317). Age was not confirmed to be an independent risk factor for AKI in our study.
Approaches to treatment should be highly individualized, with assessment of several variables. According to our findings, age should not present a contraindication for the indication of a patient for surgery.
急性肾损伤(AKI)影响大约 13%接受大腹部手术的患者,是围手术期损伤的常见且重要的临床标志。我们分析的目的是确定无已知肾脏疾病的老年患者发生 AKI 的危险因素,并评估他们的 30 天、12 个月和 5 年生存率。
我们对一组 785 例肝切除术后患者进行了回顾性分析,以确定并发症的发生率(根据 KDIGO 分类,AKI-败血症、心血管和手术并发症)。所有患者术前肾功能正常。我们确定了两组患者发生 AKI 的危险因素,按年龄分层:年龄小于 65 岁的患者和年龄大于 65 岁的患者。
年龄大于 65 岁的患者组并发症发生率明显高于年龄小于 65 岁的患者组(n=76 与 n=119;P=0.0496)。在年龄较小的患者组中,发生 AKI 的患者 30 天生存率明显较差(P=0.0004)。我们确定了 AKI 的以下独立危险因素:男性(HR 10.3834;P=0.0238)、组织学鉴定为结直肠腺癌转移(HR 2.8651;P=0.0499)、手术时间超过 300 分钟(HR 6.0096;P<0.0001)、失血量超过 500ml(HR 10.5857;P=0.0012)、术中需要超过 500ml 的新鲜冷冻血浆(HR 2.4878;P<0.0317)。在我们的研究中,年龄未被证实为 AKI 的独立危险因素。
治疗方法应高度个体化,评估多个变量。根据我们的发现,年龄不应成为患者手术适应证的禁忌症。