Department of Pneumology & Acute Respiratory Care, "Elias" Emergency University Hospital, 17 Marasti Blvd, 011461, Bucharest, Romania.
"Carol Davila" University of Medicine and Pharmacy, 8 Eroii Sanitari Blvd, 050474, Bucharest, Romania.
BMC Pulm Med. 2019 Jul 18;19(1):131. doi: 10.1186/s12890-019-0892-9.
Noninvasive ventilation (NIV) reduces the rate of endotracheal intubation (ETI) and overall mortality in severe acute exacerbation of COPD (AECOPD) with acute respiratory failure and is increasingly applied in respiratory intermediate care units. However, inadequate patient selection and incorrect management of NIV increase mortality. We aimed to identify factors that predict the outcome of NIV in AECOPD. Also, we looked for factors that influence ventilator settings and duration.
A prospective cohort study was undertaken in a respiratory intermediate care unit in an academic medical center between 2016 and 2017. Age, BMI, lung function, arterial pH and pCO2 at admission (t0), at 1-2 h (t1) and 4-6 h (t2) after admission, creatinine clearance, echocardiographic data (that defined left heart dysfunction), mean inspiratory pressure during the first 72 h (mIPAP-72 h) and hours of NIV during the first 72 h (dNIV-72 h) were recorded. Main outcome was NIV failure (i.e., ETI or in-hospital death). Secondary outcomes were in-hospital mortality, length of stay (LOS), duration of NIV (days), mIPAP-72 h, and dNIV-72 h.
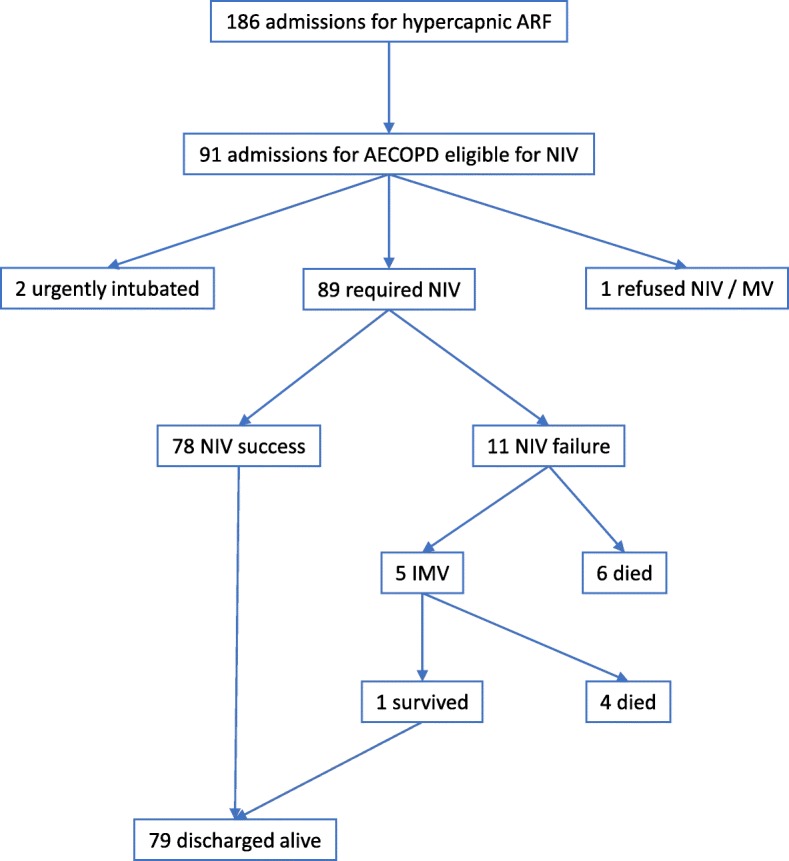
We included 89 patients (45 male, mean age 67.6 years) with AECOPD that required NIV. NIV failure was 12.4%, and in-hospital mortality was 11.2%. NIV failure was correlated with days of NIV, LOS, in-hospital mortality (p < 0.01), and kidney dysfunction (p < 0.05). In-hospital mortality was strongly associated with days of NIV (OR 1.27, 95%CI: 1.07-1.5, p < 0.01) and with FEV1 (p < 0.05). All other investigated parameters (including left heart dysfunction, dNIV-72 h, mIPAP-72 h, pH, etc.) did not influence NIV failure or mortality. dNIV-72 h and days of NIV were independent predictors of LOS (p < 0.01). Regarding the secondary outcomes, left heart dysfunction and pH at 1-2 h independently predicted NIV duration (dNIV-72 h, p < 0.01), while BMI and baseline pCO2 predicted NIV settings (mIPAP-72 h, p < 0.01).
In-hospital mortality and NIV failure were not influenced by BMI, left heart dysfunction, age, nor by arterial blood gas values in the first 6 h of NIV. Patients with severe acidosis and left heart dysfunction required prolonged use of NIV. BMI and pCO2 levels influence the NIV settings in AECOPD regardless of lung function.
无创通气(NIV)可降低伴有急性呼吸衰竭的 COPD 急性加重(AECOPD)患者的气管插管率(ETI)和总体死亡率,并在呼吸中级护理病房中得到越来越多的应用。然而,不适当的患者选择和不正确的 NIV 管理会增加死亡率。我们旨在确定预测 AECOPD 中 NIV 结果的因素。此外,我们还研究了影响呼吸机设置和持续时间的因素。
在 2016 年至 2017 年期间,在一家学术医学中心的呼吸中级护理病房进行了一项前瞻性队列研究。记录了年龄、BMI、肺功能、入院时(t0)、入院后 1-2 小时(t1)和 4-6 小时(t2)的动脉 pH 值和 pCO2、肌酐清除率、超声心动图数据(定义为左心功能障碍)、前 72 小时的平均吸气压力(mIPAP-72h)和前 72 小时的 NIV 时间(dNIV-72h)。主要结局是 NIV 失败(即 ETI 或院内死亡)。次要结局是院内死亡率、住院时间(LOS)、NIV 持续时间(天)、mIPAP-72h 和 dNIV-72h。
我们纳入了 89 例需要 NIV 的 AECOPD 患者(45 名男性,平均年龄 67.6 岁)。NIV 失败率为 12.4%,院内死亡率为 11.2%。NIV 失败与 NIV 天数、LOS、院内死亡率(p<0.01)和肾功能障碍(p<0.05)相关。院内死亡率与 NIV 天数(OR 1.27,95%CI:1.07-1.5,p<0.01)和 FEV1(p<0.05)密切相关。所有其他研究参数(包括左心功能障碍、dNIV-72h、mIPAP-72h、pH 等)均未影响 NIV 失败或死亡率。dNIV-72h 和 NIV 天数是 LOS 的独立预测因素(p<0.01)。关于次要结局,左心功能障碍和 1-2 小时时的 pH 值独立预测 NIV 持续时间(dNIV-72h,p<0.01),而 BMI 和基线 pCO2 预测 NIV 设置(mIPAP-72h,p<0.01)。
院内死亡率和 NIV 失败不受 BMI、左心功能障碍、年龄或 NIV 开始后 6 小时内的动脉血气值影响。酸中毒和左心功能障碍严重的患者需要长时间使用 NIV。BMI 和 pCO2 水平影响 AECOPD 中的 NIV 设置,而与肺功能无关。