Patel Nupur B, Jain Gaurav, Chauhan Udit, Bhadoria Ajeet Singh, Chandrakar Saurabh, Indulekha Haritha
Department of Anesthesiology and Critical Care, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
Department of Radiodiagnosis, All India Institute of Medical Sciences, Rishikesh, Uttarakhand, India.
Acute Crit Care. 2023 May;38(2):200-208. doi: 10.4266/acc.2022.01060. Epub 2023 May 25.
Baseline diaphragmatic dysfunction (DD) at the initiation of non-invasive ventilation (NIV) correlates positively with subsequent intubation. We investigated the utility of DD detected 2 hours after NIV initiation in estimating NIV failure in acute exacerbation of chronic obstructive pulmonary disease (AECOPD) patients.
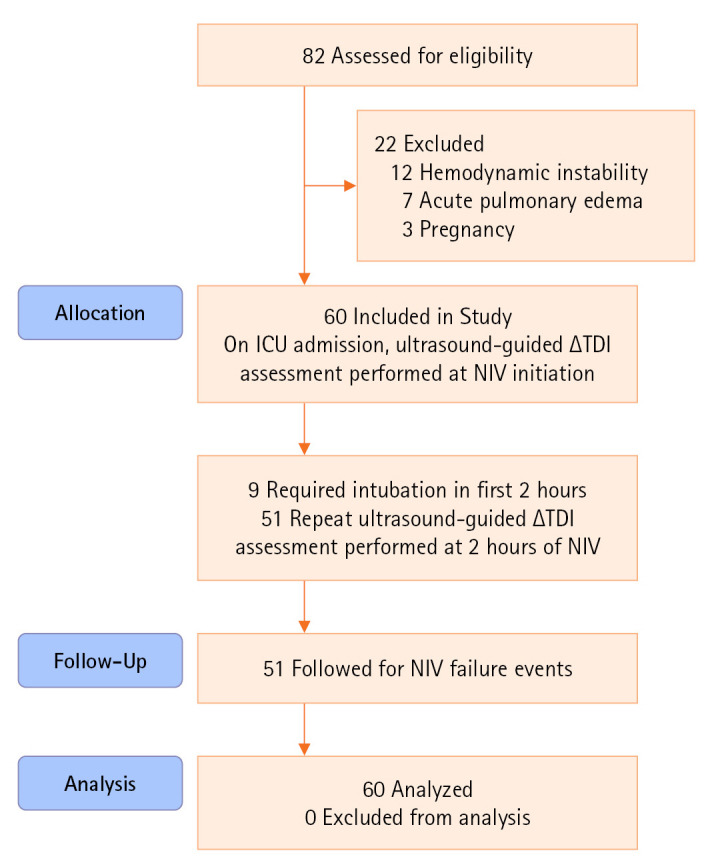
In a prospective-cohort design, we enrolled 60 consecutive patients with AECOPD initiated on NIV at intensive care unit admission, and NIV failure events were noted. The DD was assessed at baseline (T1 timepoint) and 2 hours after initiating NIV (T2 timepoint). We defined DD as ultrasound-assessed change in diaphragmatic thickness (ΔTDI) <20% (predefined criteria [PC]) or its cut-off that predicts NIV failure (calculated criteria [CC]) at both timepoints. A predictive-regression analysis was reported.
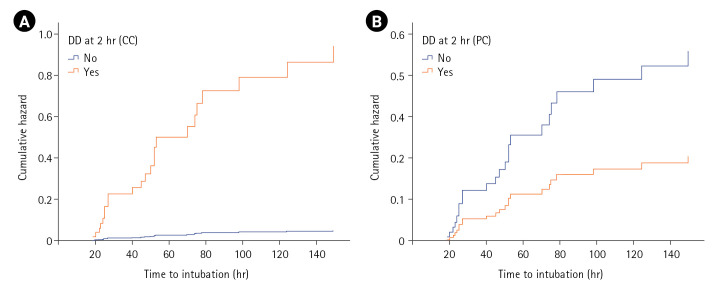
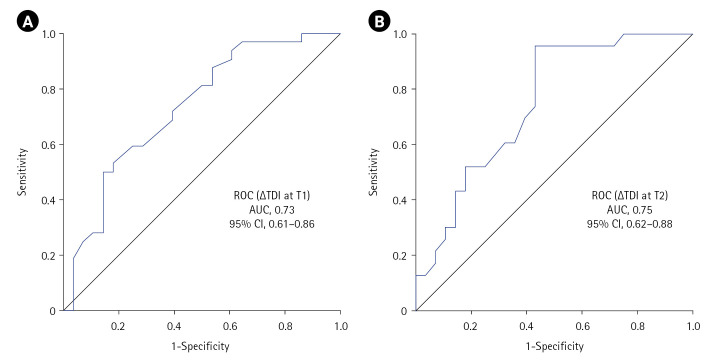
In total, 32 patients developed NIV failure, nine within 2 hours of NIV and remaining in next 6 days. The ∆TDI cut-off that predicted NIV failure (DD-CC) at T1 was ≤19.04% (area under the curve [AUC], 0.73; sensitivity, 50%; specificity, 85.71%; accuracy; 66.67%), while that at T2 was ≤35.3% (AUC, 0.75; sensitivity, 95.65%; specificity, 57.14%; accuracy, 74.51%; hazard ratio, 19.55). The NIV failure rate was 35.1% in those with normal diaphragmatic function by PC (T2) versus 5.9% by CC (T2). The odds ratio for NIV failure with DD criteria ≤35.3 and <20 at T2 was 29.33 and 4.61, while that for ≤19.04 and <20 at T1 was 6, respectively.
The DD criterion of ≤35.3 (T2) had a better diagnostic profile compared to baseline and PC in prediction of NIV failure.
无创通气(NIV)开始时的基线膈肌功能障碍(DD)与随后的插管呈正相关。我们研究了在慢性阻塞性肺疾病急性加重期(AECOPD)患者中,NIV开始2小时后检测到的DD在评估NIV失败中的效用。
采用前瞻性队列设计,我们纳入了60例在重症监护病房入院时开始接受NIV治疗的连续AECOPD患者,并记录NIV失败事件。在基线(T1时间点)和开始NIV后2小时(T2时间点)评估DD。我们将DD定义为超声评估的膈肌厚度变化(ΔTDI)<20%(预定义标准[PC])或其在两个时间点预测NIV失败的临界值(计算标准[CC])。报告了预测回归分析结果。
总共有32例患者出现NIV失败,其中9例在NIV开始后2小时内,其余在接下来的6天内。在T1时预测NIV失败的ΔTDI临界值(DD-CC)为≤19.04%(曲线下面积[AUC],0.73;敏感性,50%;特异性,85.71%;准确性,66.67%),而在T2时为≤35.3%(AUC,0.75;敏感性,95.65%;特异性,57.14%;准确性,74.51%;风险比,19.55)。根据PC(T2)膈肌功能正常的患者NIV失败率为35.1%,而根据CC(T2)为5.9%。在T2时,DD标准≤35.3且<20时NIV失败的比值比为29.33,在T1时≤19.04且<20时为6。
与基线和PC相比,≤35.3(T2)的DD标准在预测NIV失败方面具有更好的诊断特征。