Interdepartmental Division of Critical Care, University of Toronto, Toronto, Ontario, Canada.
Sunnybrook Research Institute, Department of Critical Care Medicine, Sunnybrook Health Sciences Centre, Toronto, Ontario, Canada.
JAMA Netw Open. 2019 Jul 3;2(7):e197229. doi: 10.1001/jamanetworkopen.2019.7229.
Physicians often rely on surrogate decision-makers (SDMs) to make important decisions on behalf of critically ill patients during times of incapacity. It is uncertain whether targeted interventions to improve surrogate decision-making in the intensive care unit (ICU) reduce nonbeneficial treatment and improve SDM comprehension, satisfaction, and psychological morbidity.
To perform a systematic review and meta-analysis of randomized clinical trials (RCTs) to determine the association of such interventions with patient- and family-centered outcomes and resource use.
A search was conducted of MEDLINE, Embase, and other relevant databases for potentially relevant studies from inception through May 30, 2018.
Randomized clinical trials studying interventions that were targeted at SDMs or family members of critically ill adults in the ICU were included. Key search terms included surrogate or substitute decision-maker, critically ill, randomized controlled trials, and their respective related terms.
This study followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. Two independent, blinded reviewers independently screened citations and extracted data. Random effects models with inverse variance weighting were used to pool outcomes data when possible and otherwise present findings qualitatively.
Outcomes of interest were divided into 3 categories: (1) patient-related clinical outcomes (mortality, length of stay [LOS], duration of life-sustaining therapies), (2) SDM and family-related outcomes (comprehension, major change in goals of care, incident psychological comorbidities [posttraumatic stress disorder, anxiety, depression], and satisfaction with care), and (3) use of resources (cost of care and health care resource use).
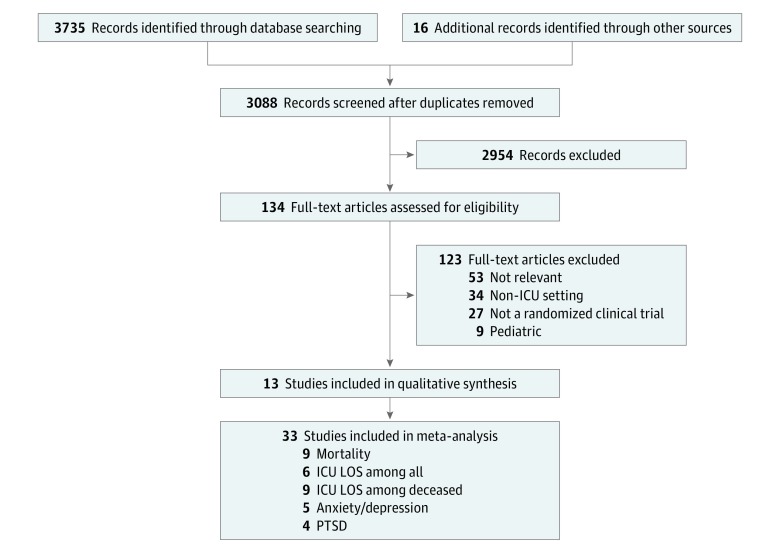
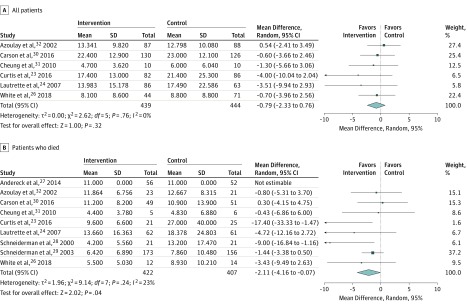
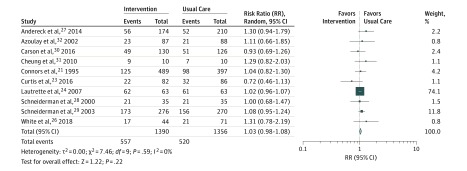
Of 3735 studies screened, 13 RCTs were included, comprising a total of 10 453 patients. Interventions were categorized as health care professional led (n = 6), ethics consultation (n = 3), palliative care consultation (n = 2), and media (n = 1 pamphlet and 1 video). No association with mortality was observed (risk ratio, 1.03; 95% CI, 0.98-1.08; P = .22). Intensive care unit LOS was significantly shorter among patients who died (mean difference, -2.11 days; 95% CI, -4.16 to -0.07; P = .04), but not in the overall population (mean difference, -0.79 days; 95% CI, -2.33 to 0.76 days; P = .32). There was no consistent difference in SDM-related outcomes, including satisfaction with care or perceived quality of care (n = 6 studies) and incident psychological comorbidities (depression: ratio of means, -0.11; 95% CI, -0.29 to 0.08; P = .26; anxiety: ratio of means, -0.08; 95% CI, -0.25 to 0.08; P = .31; or posttraumatic stress disorder: ratio of means: -0.04; 95% CI, -0.21 to 0.13; P = .65). Among 6 trials reporting effects on health care resource use, only 1 nurse-led intervention observed a significant reduction in costs ($75 850 control vs $51 060 intervention; P = .04).
Systematic interventions aimed at improving surrogate decision-making for critically ill adults may reduce ICU LOS among patients who die in the ICU, without influencing overall mortality. Better understanding of the complex processes related to surrogate decision-making is needed.
医生在患者丧失能力时经常依靠代理人(SDM)代表重病患者做出重要决定。目前尚不确定在重症监护病房(ICU)中针对改善代理决策的靶向干预是否会减少无益的治疗并改善 SDM 的理解、满意度和心理发病率。
进行系统评价和荟萃分析随机临床试验(RCT),以确定此类干预措施与以患者和家庭为中心的结局以及资源使用之间的关联。
对 MEDLINE、Embase 和其他相关数据库进行了搜索,以确定从开始到 2018 年 5 月 30 日可能相关的研究。
纳入了针对 ICU 中成年重症患者的 SDM 或其家庭成员的干预措施进行研究的随机临床试验。关键搜索词包括替代或替代决策制定者、重症、随机对照试验及其各自的相关术语。
本研究遵循系统评价和荟萃分析的首选报告项目(PRISMA)指南。两名独立的、盲目的评审员独立筛选引文并提取数据。当可能时,使用具有逆方差加权的随机效应模型来汇总结果数据,否则以定性方式呈现发现。
感兴趣的结果分为 3 类:(1)患者相关的临床结局(死亡率、住院时间 [LOS]、生命维持治疗的持续时间),(2)SDM 和家庭相关的结局(理解、治疗目标的重大变化、发生的心理合并症[创伤后应激障碍、焦虑、抑郁]和对护理的满意度),以及(3)资源使用(护理成本和医疗保健资源使用)。
在筛选出的 3735 项研究中,纳入了 13 项 RCT,共纳入了 10453 名患者。干预措施分为医疗保健专业人员主导(n=6)、伦理咨询(n=3)、姑息治疗咨询(n=2)和媒体(n=1 小册子和 1 视频)。未观察到死亡率的相关性(风险比,1.03;95%CI,0.98-1.08;P=0.22)。死亡患者的 ICU LOS 显著缩短(平均差异,-2.11 天;95%CI,-4.16 至-0.07;P=0.04),但在总体人群中则不然(平均差异,-0.79 天;95%CI,-2.33 至 0.76 天;P=0.32)。在 SDM 相关结局方面,包括对护理的满意度或感知到的护理质量(n=6 项研究)和发生的心理合并症(抑郁:均数比,-0.11;95%CI,-0.29 至 0.08;P=0.26;焦虑:均数比,-0.08;95%CI,-0.25 至 0.08;P=0.31;或创伤后应激障碍:均数比:-0.04;95%CI,-0.21 至 0.13;P=0.65),没有一致的差异。在报告对卫生保健资源使用影响的 6 项试验中,只有 1 项护士主导的干预措施观察到成本显著降低(对照组 75850 美元 vs 干预组 51060 美元;P=0.04)。
针对重症成人改善代理决策的系统干预措施可能会减少 ICU 中死亡患者的 ICU LOS,而不会影响整体死亡率。需要更好地了解与代理决策相关的复杂过程。