Division of Hematology, Respiratory Medicine and Oncology, Faculty of Medicine, Saga University, Saga, Japan.
Thorac Cancer. 2019 Sep;10(9):1798-1804. doi: 10.1111/1759-7714.13149. Epub 2019 Jul 22.
Immune-related adverse events (irAEs) should be anticipated with treatment by immune checkpoint inhibitors (ICIs). Although the relationship between irAEs and efficacy of ICI has been reported, it has not yet been clarified whether the benefit from ICI outweighs the low frequency of proceeding to subsequent therapies after discontinuation due to irAEs.
The study comprised 61 patients with non-small cell lung cancer who underwent treatment with ICIs (nivolumab or pembrolizumab monotherapy) at the Saga University Medical School Hospital from December 2015 to January 2018. Therapeutic effect and progression-free survival (PFS) were compared between the irAEs discontinuation group (AEg) and the group with discontinuation due to all causes other than irAEs (Non-AEg).
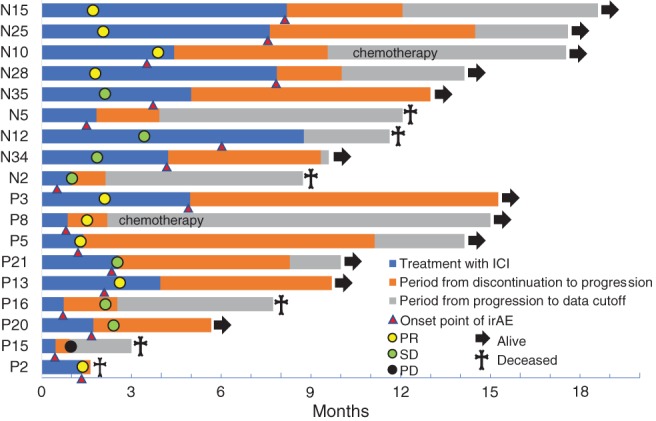
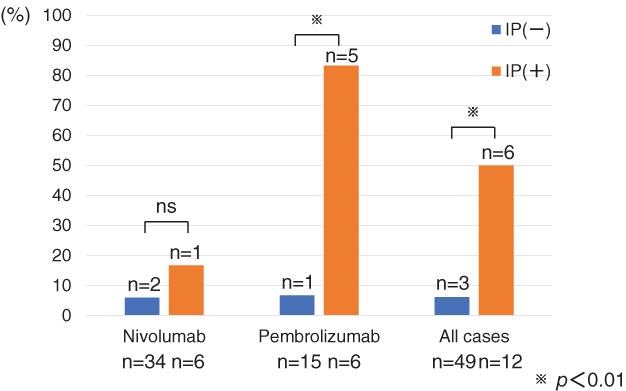
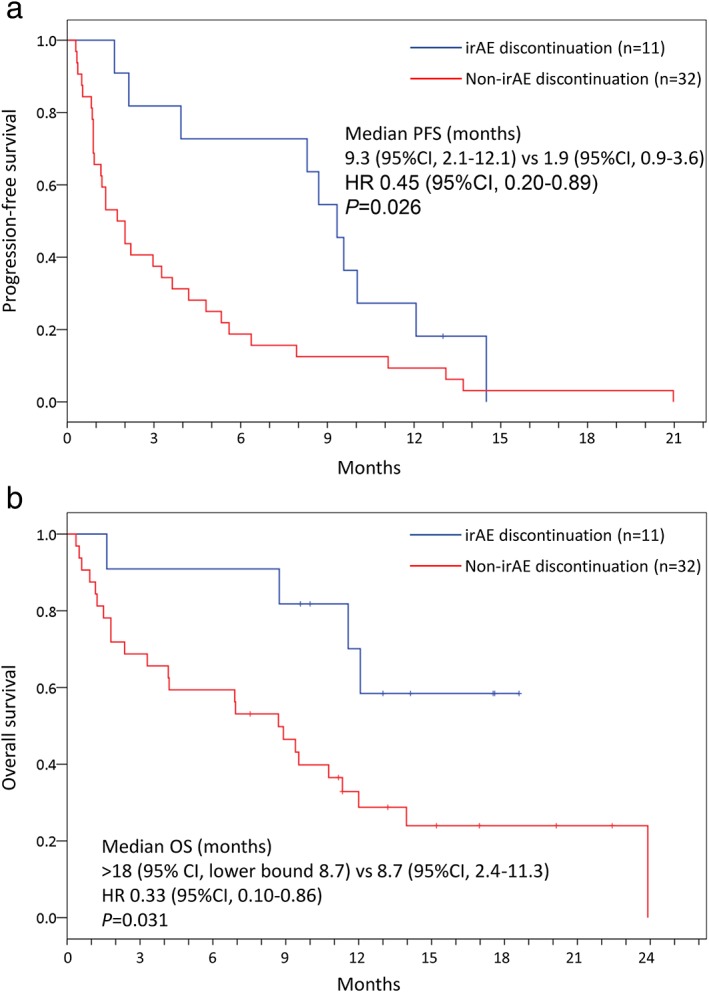
A total of 30% patients(18/61) had therapy discontinued due to irAEs: 22.5% (9/40) with nivolumab and 42.9% (9/21) with pembrolizumab. The response rate was 50.0% in the AEg and 8.1% in the on-AEg (P = 0.001). The median PFS was significantly longer in the AEg (9.3 months; 95% CI 2.1-12.1) than in the non-AEg (1.9 months; 95% CI 0.9-3.6): HR 0.45 (95%CI 0.20-0.89; log-rank test P = 0.026). The prevalence of drug-induced interstitial lung disease (ILD) was 6.1% (3/49) in cases without interstitial pneumonia (IP) as the underlying disease, whereas it was 50% (6/12) in cases with IP (P = 0.001).
Discontinuation of treatment with ICIs due to irAEs predict a good response to ICIs and favorable outcome since their anti-cancer effects continue even after discontinuation. However, the presence of IP as the underlying disease increases the risk of drug-related ILD onset.
免疫相关不良事件(irAEs)在接受免疫检查点抑制剂(ICI)治疗时应有所预期。虽然已经报道了 irAEs 与 ICI 疗效之间的关系,但尚未阐明由于 irAEs 而停止治疗后,继续进行后续治疗的频率较低是否会带来益处。
本研究纳入了 2015 年 12 月至 2018 年 1 月在佐贺大学医学院医院接受 ICI(nivolumab 或 pembrolizumab 单药治疗)的 61 例非小细胞肺癌患者。比较了 irAEs 停药组(AEg)和因非 irAEs 原因停药组(非-AEg)的治疗效果和无进展生存期(PFS)。
共有 30%的患者(18/61)因 irAEs 而停止治疗:nivolumab 组为 22.5%(9/40),pembrolizumab 组为 42.9%(9/21)。AEg 的缓解率为 50.0%,非-AEg 为 8.1%(P=0.001)。AEg 的中位 PFS 明显长于非-AEg(9.3 个月;95%CI 2.1-12.1):HR 0.45(95%CI 0.20-0.89;log-rank 检验 P=0.026)。无间质性肺炎(IP)基础疾病的病例中,药物性间质性肺病(ILD)的发生率为 6.1%(3/49),而有 IP 基础疾病的病例中为 50%(6/12)(P=0.001)。
由于 irAEs 而停止使用 ICI 治疗可预测对 ICI 的良好反应和有利的结果,因为即使停药后其抗癌作用仍在继续。然而,存在 IP 作为基础疾病会增加药物相关 ILD 发病的风险。