Department of Respiratory Medicine, Children's Health Queensland, South Brisbane, Australia.
Centre for Children's Health Research, Brisbane, Australia.
Pediatr Pulmonol. 2019 Nov;54(11):1774-1780. doi: 10.1002/ppul.24455. Epub 2019 Jul 21.
Spinal muscular atrophy (SMA) causes progressive respiratory muscle weakness but respiratory function (RF) in those using noninvasive ventilation (NIV) is not well described.
To describe RF in childhood SMA and assess differences between those using and not using NIV.
A cross-sectional study of childhood SMA assessed polysomnography (PSG), spirometry, forced oscillation technique (FOT), lung clearance index (LCI), sniff nasal inspiratory pressures, peak cough flow, maximal inspiratory and expiratory pressure, and NIV use and indication.
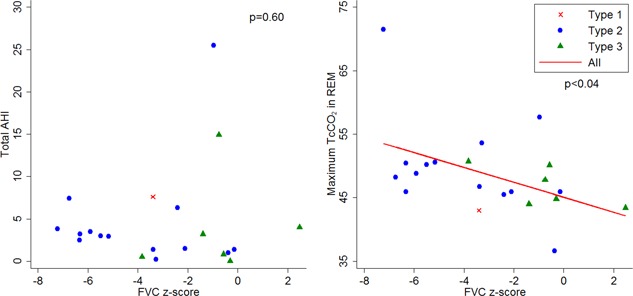
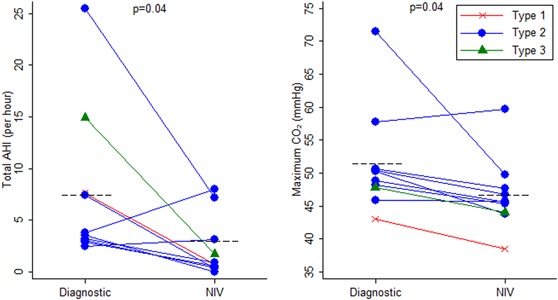
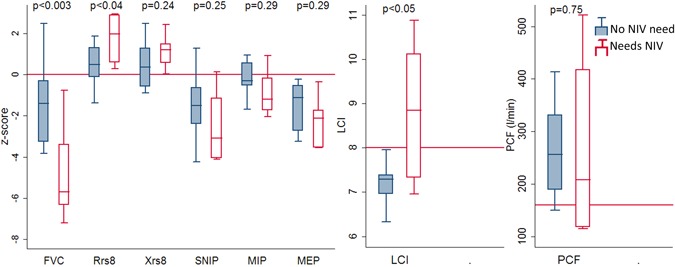
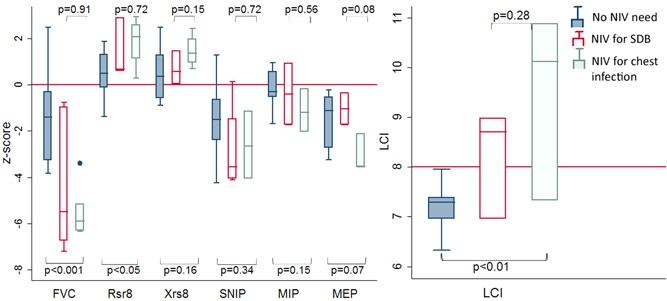
Twenty-five children (median age [interquartile range], 8.96 [5.63] years; 10 F) with SMA 1 (n = 3), 2 (n = 15), and 3 (n = 7) were recruited. Spirometry and FOT testing was feasible in children as young as 3 years. Ten (40%) required NIV, 5 for sleep-disordered breathing (SDB), and 5 initiated during lower respiratory tract infection (LRTI). Children requiring NIV were older (median, 10.52 vs 5.67 years; P < .02) with more abnormal forced vital capacity (FVC) z-score (-5.70 vs -1.39, P < .02), Rsr8 z-score (1.97 vs 0.50, P = .04), and LCI (8.84 vs 7.34, P = .01). Two had normal RF and SDB. For FVC z-score less than -2.5 and LCI greater than 7.5, the odds ratio for NIV was 10.70 (95% confidence interval [CI], 1.39-82.03) and 2 (95% CI, 0.40-10.31), respectively. All children with LCI greater than 8 used NIV. FVC z-score and LCI are associated with maximum transcutaneous carbon dioxide on PSG (r = 0.43, P < .001).
NIV is common in SMA. Normal RF does not exclude SDB. Children with more abnormal FVC and LCI should be considered at risk of starting NIV during/following an LRTI.
脊髓性肌萎缩症(SMA)导致进行性呼吸肌无力,但使用无创通气(NIV)的患者的呼吸功能(RF)尚未得到很好的描述。
描述儿童 SMA 的 RF,并评估使用和不使用 NIV 的患者之间的差异。
采用横断面研究方法,评估了儿童 SMA 的多导睡眠图(PSG)、肺量计、强迫振荡技术(FOT)、肺清除指数(LCI)、嗅探鼻吸气压力、最大咳嗽流量、最大吸气和呼气压力,以及 NIV 的使用和适应证。
共招募了 25 名 SMA 1 型(n=3)、2 型(n=15)和 3 型(n=7)的儿童(中位年龄[四分位数范围],8.96[5.63]岁;10 名女性)。年龄在 3 岁以下的儿童也可进行肺量计和 FOT 检测。10 名(40%)需要 NIV,5 名用于睡眠呼吸障碍(SDB),5 名在下呼吸道感染(LRTI)期间开始使用。需要 NIV 的儿童年龄较大(中位数分别为 10.52 岁和 5.67 岁;P<.02),用力肺活量(FVC)z 评分更差(-5.70 与-1.39,P<.02)、Rsr8 z 评分(1.97 与 0.50,P=.04)和 LCI 更高(8.84 与 7.34,P=.01)。其中 2 名儿童的 RF 和 SDB 正常。对于 FVC z 评分小于-2.5 和 LCI 大于 7.5,NIV 的比值比为 10.70(95%置信区间[CI],1.39-82.03)和 2(95%CI,0.40-10.31)。所有 LCI 大于 8 的儿童均使用 NIV。FVC z 评分和 LCI 与 PSG 上最大经皮二氧化碳分压(r=0.43,P<.001)相关。
SMA 患者中 NIV 很常见。正常的 RF 并不能排除 SDB。FVC 和 LCI 异常更明显的儿童在 LRTI 期间/之后开始使用 NIV 的风险应更高。