Department of Health Research Methods, Evidence and Impact, McMaster University, Hamilton, ON, Canada.
Department of Obstetrics and Gynaecology, Faculty of Medicines and Biomedical Sciences University of Yaounde 1, Yaoundé, Cameroon.
BMC Pregnancy Childbirth. 2019 Jul 22;19(1):257. doi: 10.1186/s12884-019-2407-3.
There is some evidence that suggests misoprostol may supplement the action of oxytocin in preventing post-partum haemorrhage (PPH). The primary objective of this study was to determine the effect of the administration of 600 μg misoprostol in addition to oxytocin versus oxytocin alone, on the risk of PPH among pregnant women after delivery. The secondary objectives were to determine the effects of the above combination on maternal death and blood transfusion among pregnant women after delivery; and to determine the incidence of PPH, its case fatality, and the maternal mortality ratio in our hospital.
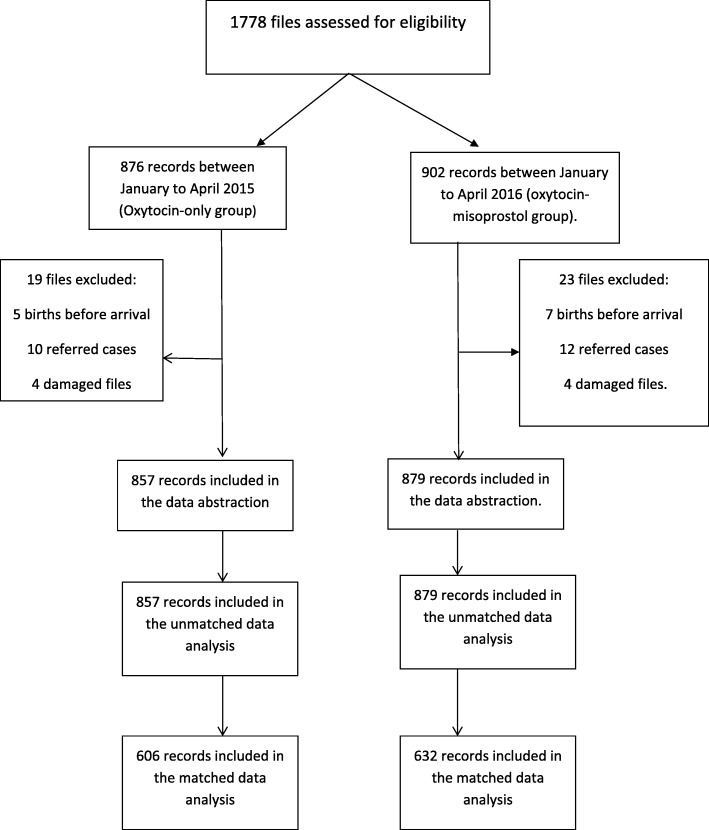
Design and setting: Retrospective chart review of 1736 women delivering at the Regional Hospital Bamenda Cameroon, between 2015 and 2016. This was a pre versus post study following a policy change in the prevention of PPH. Exposure groups: One group received oxytocin-misoprostol (January-April 2016: period after policy change), and the second group received oxytocin-only (January-April 2015: period before policy change) after delivery.
The primary outcome was PPH, and the secondary outcomes were maternal death and blood transfusion.
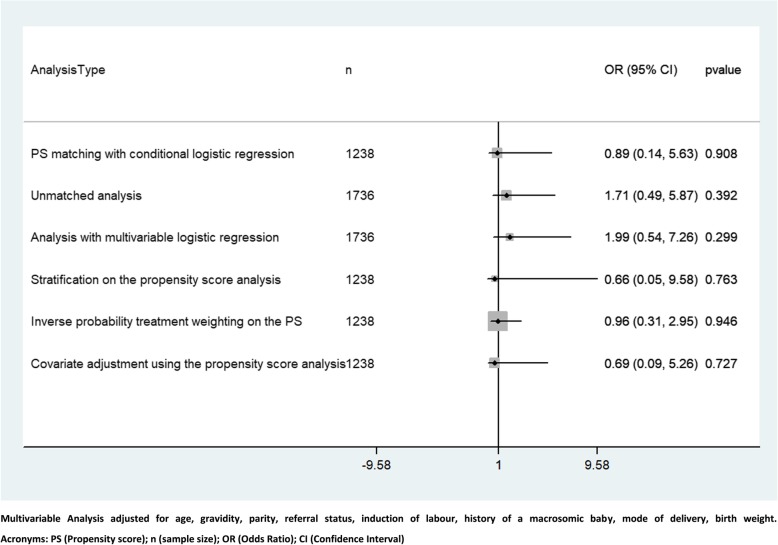
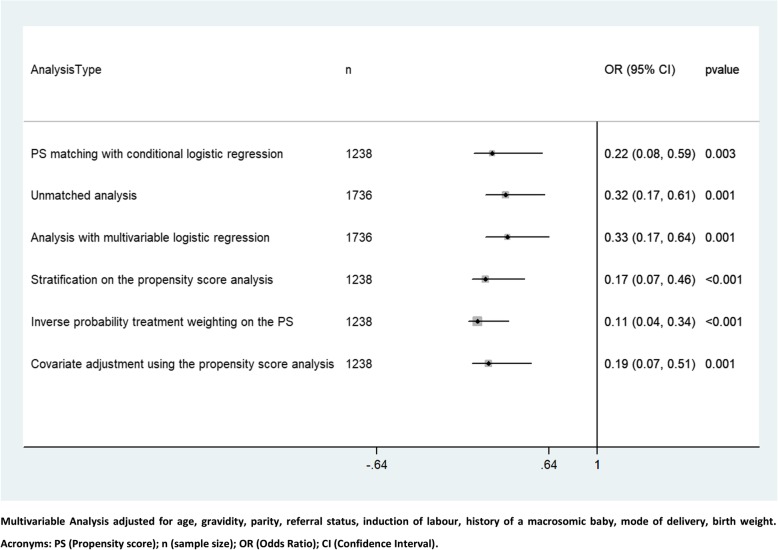
A 1:1 matching with replacement was done with the propensity score (PS). The groups were compared using PS matching with conditional logistic regression on the matched pairs as the main analysis. A sensitivity analysis was done using other PS adjustment methods and multiple regression.
Of the 1736 women included in this study, 1238 were matched and compared. Women who received oxytocin-misoprostol were less likely to have PPH as compared to those receiving oxytocin-only (odds ratio [OR] 0.22, 95% confidence interval [CI] 0.08, 0.59, p = 0.003). This reduced odds of PPH was upheld in the different sensitivity analyses. There were no significant differences in the odds of maternal death and the use of blood transfusions between the two groups: OR 3.91, 95% CI [0.44, 35.08], p = 0.22, and OR 0.89, 95% CI [0.14-5.63], p = 0.91, respectively. Sensitivity analyses showed similar results. The incidence of PPH was 2.9% (before adding misoprostol the incidence was 4.4% and after adding misoprostol it was 1.5%), the case fatality rate of PPH was 1.96%, and the overall maternal mortality ratio in the hospital was 293 maternal deaths/100000 life births.
Our evidence suggests that using 600 μg misoprostol as an add-on to oxytocin in the prevention of post-partum haemorrhage significantly reduces the odds of PPH without affecting other maternal outcomes.
有证据表明,米索前列醇可能会补充催产素在预防产后出血(PPH)方面的作用。本研究的主要目的是确定在产妇分娩后给予 600μg米索前列醇联合催产素与单独使用催产素相比,对 PPH 风险的影响。次要目的是确定上述联合用药对产妇分娩后死亡和输血的影响;并确定我们医院的 PPH 发生率、病死率和孕产妇死亡率。
设计和设置:对喀麦隆巴门达地区医院 2015 年至 2016 年期间分娩的 1736 名妇女进行回顾性图表审查。这是一项预防 PPH 的政策改变后的前瞻性研究。暴露组:一组接受催产素-米索前列醇(2016 年 1 月至 4 月:政策改变后),另一组仅接受催产素(2015 年 1 月至 4 月:政策改变前)。
主要结局为 PPH,次要结局为产妇死亡和输血。
采用倾向评分(PS)进行 1:1 匹配替换。使用条件逻辑回归对匹配对进行 PS 匹配比较,作为主要分析。使用其他 PS 调整方法和多元回归进行敏感性分析。
在这项研究的 1736 名妇女中,有 1238 名进行了匹配比较。与仅接受催产素的妇女相比,接受催产素-米索前列醇的妇女发生 PPH 的可能性较低(比值比[OR]0.22,95%置信区间[CI]0.08,0.59,p=0.003)。这一降低 PPH 的可能性在不同的敏感性分析中得到了支持。两组间产妇死亡和输血的可能性无显著差异:OR 3.91,95%CI[0.44,35.08],p=0.22,和 OR 0.89,95%CI[0.14-5.63],p=0.91。敏感性分析也得出了类似的结果。PPH 的发生率为 2.9%(添加米索前列醇前的发生率为 4.4%,添加米索前列醇后的发生率为 1.5%),PPH 的病死率为 1.96%,医院的总体孕产妇死亡率为 293 例孕产妇死亡/100000 例活产。
我们的证据表明,在预防产后出血时,将 600μg米索前列醇作为催产素的附加药物使用,可显著降低 PPH 的发生几率,而不影响其他产妇结局。