Lunenfeld Bruno, Bilger Wilma, Longobardi Salvatore, Alam Veronica, D'Hooghe Thomas, Sunkara Sesh K
Faculty of Life Sciences, Bar-Ilan University, Ramat Gan, Israel.
Medical Affairs Fertility, Endocrinology and General Medicine, Merck Serono GmbH, Darmstadt, Germany.
Front Endocrinol (Lausanne). 2019 Jul 3;10:429. doi: 10.3389/fendo.2019.00429. eCollection 2019.
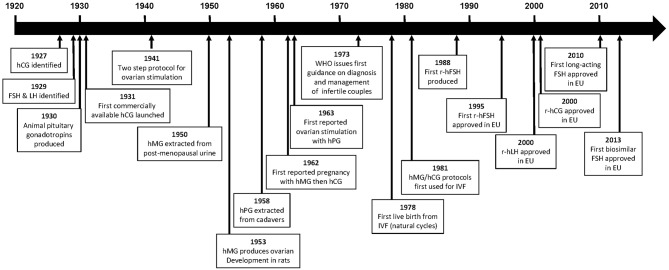
The first commercially available gonadotropin product was a human chorionic gonadotropin (hCG) extract, followed by animal pituitary gonadotropin extracts. These extracts were effective, leading to the introduction of the two-step protocol, which involved ovarian stimulation using animal gonadotropins followed by ovulation triggering using hCG. However, ovarian response to animal gonadotropins was maintained for only a short period of time due to immune recognition. This prompted the development of human pituitary gonadotropins; however, supply problems, the risk for Creutzfeld-Jakob disease, and the advent of recombinant technology eventually led to the withdrawal of human pituitary gonadotropin from the market. Urinary human menopausal gonadotropin (hMG) preparations were also produced, with subsequent improvements in purification techniques enabling development of products with standardized proportions of follicle-stimulating hormone (FSH) and luteinizing hormone (LH) activity. In 1962 the first reported pregnancy following ovulation stimulation with hMG and ovulation induction with hCG was described, and this product was later established as part of the standard protocol for ART. Improvements in immunopurification techniques enabled the removal of LH from hMG preparations; however, unidentified urinary protein contaminants remained a problem. Subsequently, monoclonal FSH antibodies were used to produce a highly purified FSH preparation containing <0.1 IU of LH activity and <5% unidentified urinary proteins, enabling the formulation of smaller injection volumes that could be administered subcutaneously rather than intramuscularly. Ongoing issues with gonadotropins derived from urine donations, including batch-to-batch variability and a finite donor supply, were overcome by the development of recombinant gonadotropin products. The first recombinant human FSH molecules received marketing approvals in 1995 (follitropin alfa) and 1996 (follitropin beta). These had superior purity and a more homogenous glycosylation pattern compared with urinary or pituitary FSH. Subsequently recombinant versions of LH and hCG have been developed, and biosimilar versions of follitropin alfa have received marketing authorization. More recent developments include a recombinant FSH produced using a human cell line, and a long-acting FSH preparation. These state of the art products are administered subcutaneously via pen injection devices.
首个上市的促性腺激素产品是一种人绒毛膜促性腺激素(hCG)提取物,随后是动物垂体促性腺激素提取物。这些提取物有效,促使两步方案的引入,该方案包括使用动物促性腺激素刺激卵巢,随后使用hCG触发排卵。然而,由于免疫识别,卵巢对动物促性腺激素的反应仅维持较短时间。这促使了人垂体促性腺激素的研发;然而,供应问题、克雅氏病风险以及重组技术的出现最终导致人垂体促性腺激素退出市场。还生产了尿促性素(hMG)制剂,随后纯化技术的改进使得能够开发出具有标准化促卵泡激素(FSH)和促黄体生成素(LH)活性比例的产品。1962年首次报道了用hMG刺激排卵并用hCG诱导排卵后怀孕的情况,该产品后来成为辅助生殖技术标准方案的一部分。免疫纯化技术的改进使得能够从hMG制剂中去除LH;然而,未鉴定的尿蛋白污染物仍然是个问题。随后,单克隆FSH抗体被用于生产一种高度纯化的FSH制剂,其LH活性<0.1 IU,未鉴定的尿蛋白<5%,使得能够配制可皮下而非肌肉注射的更小注射体积。来自尿液捐赠的促性腺激素持续存在的问题,包括批次间差异和有限的供体供应,通过重组促性腺激素产品的开发得到了克服。首个重组人FSH分子于1995年(重组促卵泡素α)和1996年(重组促卵泡素β)获得上市批准。与尿源性或垂体源性FSH相比,这些产品具有更高的纯度和更均匀的糖基化模式。随后开发了LH和hCG的重组版本,重组促卵泡素α的生物类似药也获得了上市授权。最近的进展包括使用人细胞系生产的重组FSH以及长效FSH制剂。这些先进产品通过笔式注射装置皮下给药。