Mező Blanka, Heilos Andreas, Böhmig Georg A, Eskandary Farsad, Wahrmann Markus, Bond Gregor, Kozakowski Nicolas, Halloran Philip F, Rusai Krisztina, Prohászka Zoltán
IIIrd Department of Internal Medicine and MTA-SE Research Group of Immunology and Hematology, Research Laboratory, Hungarian Academy of Sciences and Semmelweis University, Budapest, Hungary.
Department of Pediatrics and Adolescent Medicine, Medical University of Vienna, Vienna, Austria.
Transplant Direct. 2019 Jun 27;5(7):e470. doi: 10.1097/TXD.0000000000000915. eCollection 2019 Jul.
Antibody-mediated rejection (AMR) is a major cause of kidney allograft failure. Its molecular mechanisms are multifaceted and may include a role of complement activation via the classical pathway. Here, we investigated whether noninvasive complement monitoring adds predictive power to the diagnosis of AMR in the setting of donor-specific antibody (DSA) positivity.
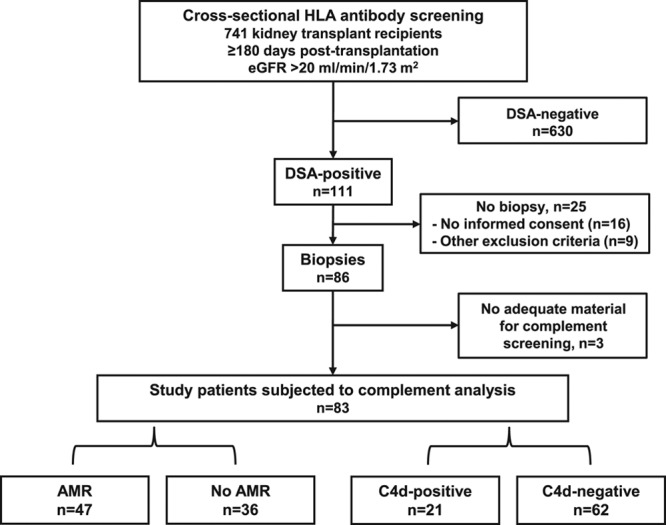
In this cross-sectional study, 741 kidney transplant recipients with stable graft function ≥180 days posttransplantation were screened for the presence of human leukocyte antigen (HLA) alloantibodies. Eighty-three of 111 DSA-positive recipients underwent protocol biopsies and were tested for blood and urinary levels of complement proteins (C1q, C4, C3) and activation products (C4d, C3a, C5a, C5b-9).
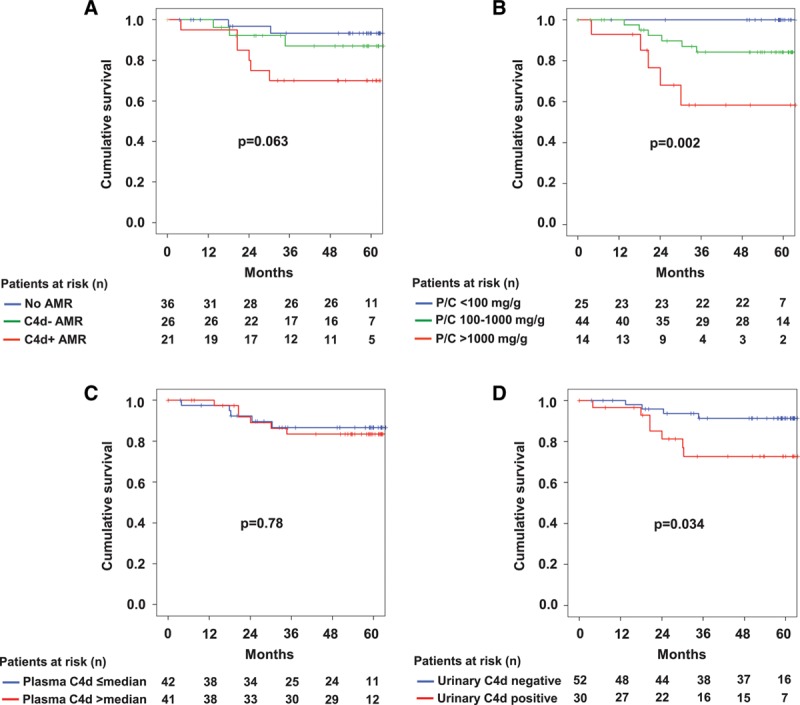
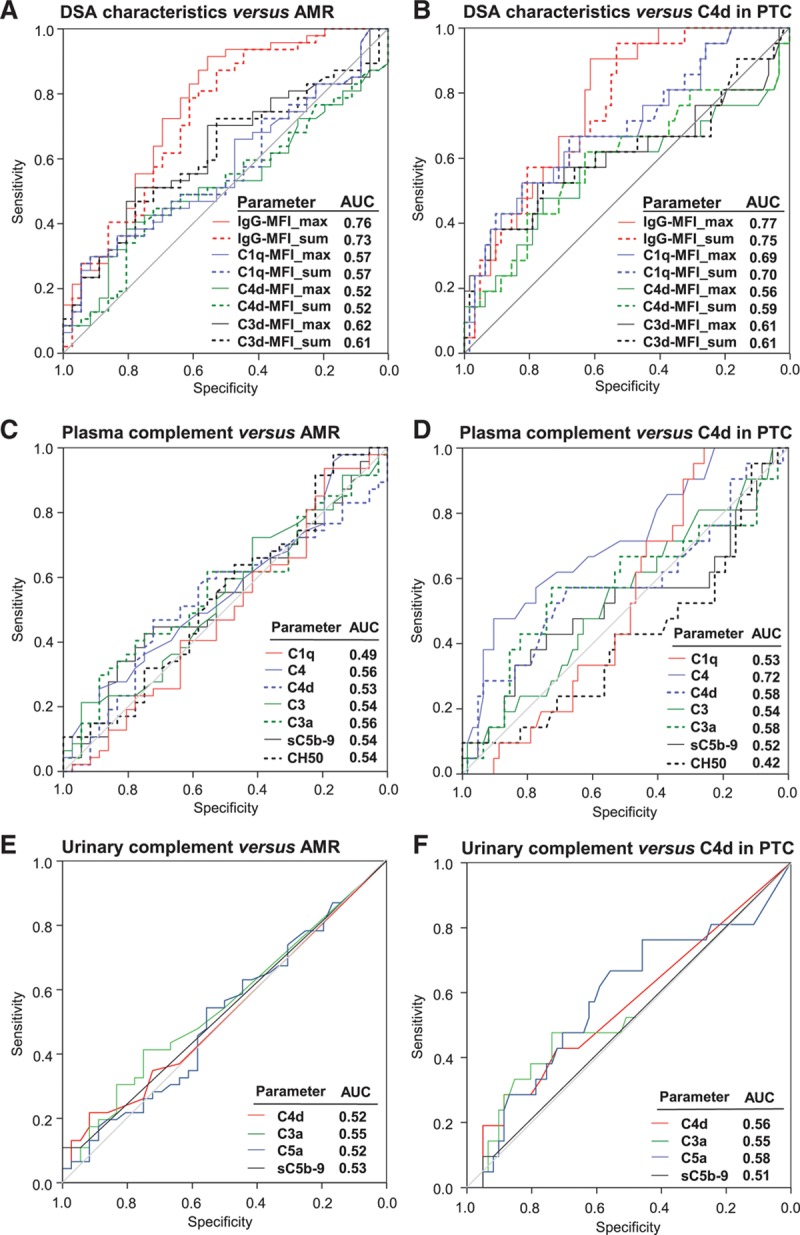
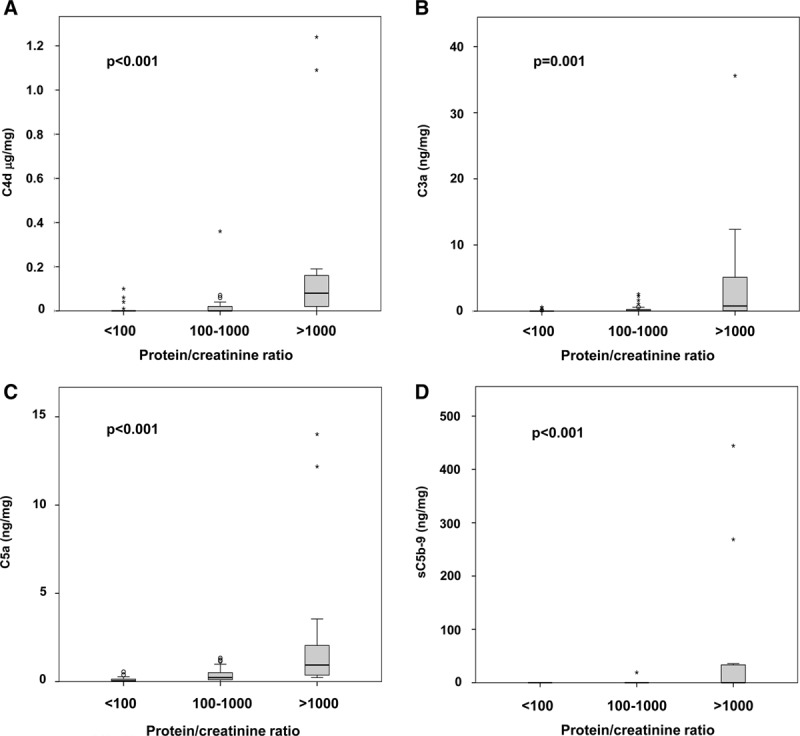
Forty-seven recipients were diagnosed with AMR, and 21 were C4d-positive. While biopsy-confirmed AMR (and C4d) associated with DSA-binding strength (IgG mean fluorescence intensity of the immunodominant DSA versus AMR; area under the receiver operating characteristic curve: 0.76), tested complement markers did not have any predictive value for rejection (area under the receiver operating characteristic curve: 0.49-0.56). There were, however, tight correlations between complement activation products in urine and protein/creatinine ratio ( = 0.44-0.64; < 0.001). Analysis of death-censored graft survival over a median of 60 months revealed no independent associations with levels of complement markers in blood or urine.
Complement patterns in blood and urine failed to identify AMR in late biopsies and may have no relevant diagnostic value in this particular context.
抗体介导的排斥反应(AMR)是肾移植失败的主要原因。其分子机制是多方面的,可能包括经典途径补体激活的作用。在此,我们研究了在供体特异性抗体(DSA)阳性的情况下,非侵入性补体监测是否能增强对AMR诊断的预测能力。
在这项横断面研究中,对741例移植后肾功能稳定≥180天的肾移植受者进行了人类白细胞抗原(HLA)同种抗体筛查。111例DSA阳性受者中的83例接受了方案活检,并检测了血液和尿液中补体蛋白(C1q、C4、C3)和激活产物(C4d、C3a、C5a、C5b-9)的水平。
47例受者被诊断为AMR,21例C4d阳性。虽然活检确诊的AMR(和C4d)与DSA结合强度相关(免疫显性DSA的IgG平均荧光强度与AMR;受试者操作特征曲线下面积:0.76),但检测的补体标志物对排斥反应没有任何预测价值(受试者操作特征曲线下面积:0.49-0.56)。然而,尿液中的补体激活产物与蛋白/肌酐比值之间存在密切相关性(r=0.44-0.64;P<0.001)。对中位60个月的死亡删失移植肾存活情况分析显示,与血液或尿液中的补体标志物水平无独立相关性。
血液和尿液中的补体模式未能在晚期活检中识别出AMR,在这种特定情况下可能没有相关诊断价值。