van Veldhuisen Eran, van den Oord Claudia, Brada Lilly J, Walma Marieke S, Vogel Jantien A, Wilmink Johanna W, Del Chiaro Marco, van Lienden Krijn P, Meijerink Martijn R, van Tienhoven Geertjan, Hackert Thilo, Wolfgang Christopher L, van Santvoort Hjalmar, Groot Koerkamp Bas, Busch Olivier R, Molenaar I Quintus, van Eijck Casper H, Besselink Marc G
Department of Surgery, Cancer Center Amsterdam, Amsterdam UMC, University of Amsterdam, 1105 AZ Amsterdam, The Netherlands.
Department of Surgery, Regional Academic Cancer Center Utrecht, University of Utrecht, 3584 CX Utrecht, The Netherlands.
Cancers (Basel). 2019 Jul 12;11(7):976. doi: 10.3390/cancers11070976.
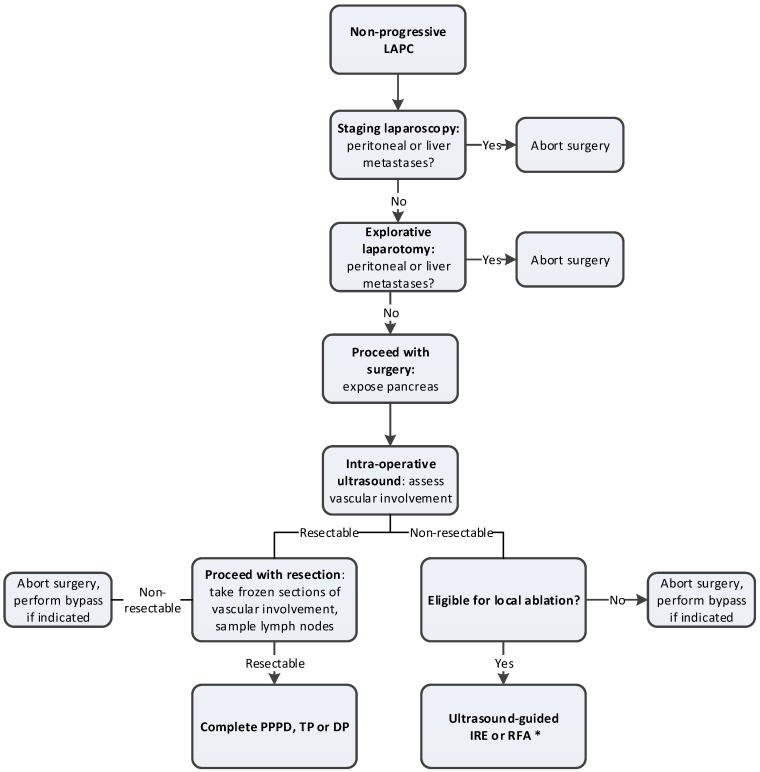
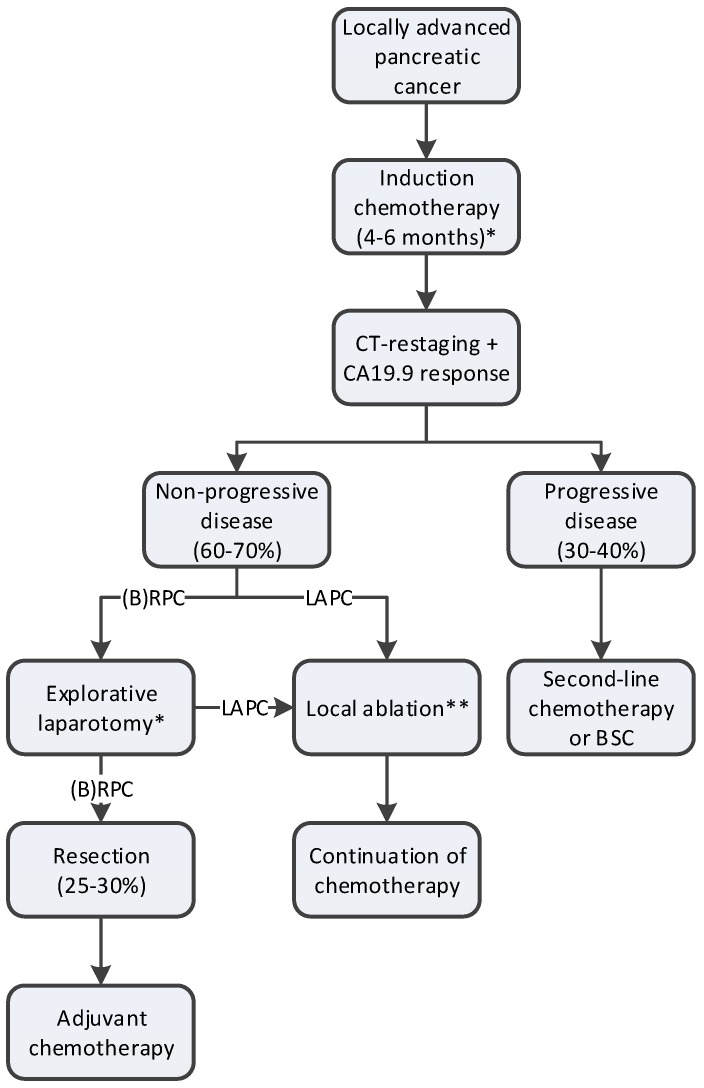
Locally advanced pancreatic cancer (LAPC) has several definitions but essentially is a nonmetastasized pancreatic cancer, in which upfront resection is considered not beneficial due to extensive vascular involvement and consequent high chance of a nonradical resection. The introduction of FOLFIRINOX chemotherapy and gemcitabine-nab-paclitaxel (gem-nab) has had major implications for the management and outcome of patients with LAPC. After 4-6 months induction chemotherapy, the majority of patients have stable disease or even tumor-regression. Of these, 12 to 35% are successfully downstaged to resectable disease. Several studies have reported a 30-35 months overall survival after resection; although it currently remains unclear if this is a result of the resection or the good response to chemotherapy. Following chemotherapy, selection of patients for resection is difficult, as contrast-enhanced computed-tomography (CT) scan is unreliable in differentiating between viable tumor and fibrosis. In case a resection is not considered possible but stable disease is observed, local ablative techniques are being studied, such as irreversible electroporation, radiofrequency ablation, and stereotactic body radiation therapy. Pragmatic, multicenter, randomized studies will ultimately have to confirm the exact role of both surgical exploration and ablation in these patients. Since evidence-based guidelines for the management of LAPC are lacking, this review proposes a standardized approach for the treatment of LAPC based on the best available evidence.
局部进展期胰腺癌(LAPC)有多种定义,但本质上是一种未发生转移的胰腺癌,由于广泛的血管受累以及随之而来的非根治性切除的高概率,术前切除被认为没有益处。FOLFIRINOX化疗和吉西他滨-纳米白蛋白结合型紫杉醇(吉西他滨-纳米紫杉醇)的引入对LAPC患者的管理和预后产生了重大影响。经过4至6个月的诱导化疗,大多数患者病情稳定甚至肿瘤缩小。其中,12%至35%的患者成功降期为可切除疾病。多项研究报告称,切除术后总生存期为30至35个月;尽管目前尚不清楚这是切除的结果还是对化疗的良好反应。化疗后,选择切除患者很困难,因为对比增强计算机断层扫描(CT)在区分存活肿瘤和纤维化方面不可靠。如果认为无法进行切除但观察到病情稳定,则正在研究局部消融技术,如不可逆电穿孔、射频消融和立体定向体部放射治疗。务实的多中心随机研究最终必须证实手术探查和消融在这些患者中的确切作用。由于缺乏基于证据的LAPC管理指南,本综述基于现有最佳证据提出了一种标准化的LAPC治疗方法。