Community and Primary Care Research Group, University of Plymouth, Plymouth, UK.
Sociology, Philosophy and Anthropology Department, University of Exeter, Exeter, UK.
BMJ Open. 2019 Jul 23;9(7):e029721. doi: 10.1136/bmjopen-2019-029721.
To evaluate a county-wide deincentivisation of the Quality and Outcomes Framework (QOF) payment scheme for UK General Practice (GP).
In 2014, National Health Service England signalled a move towards devolution of QOF to Clinical Commissioning Groups. Fifty-five GPs in Somerset established the Somerset Practice Quality Scheme (SPQS)-a deincentivisation of QOF-with the goal of redirecting resources towards Person Centred Coordinated Care (P3C), especially for those with long-term conditions (LTCs). We evaluated the impact on processes and outcomes of care from April 2016 to March 2017.
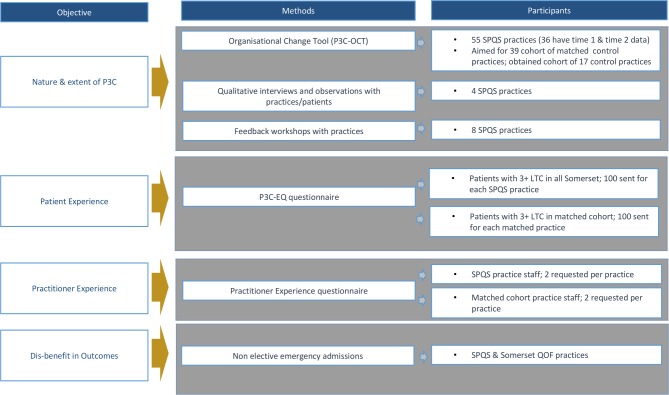
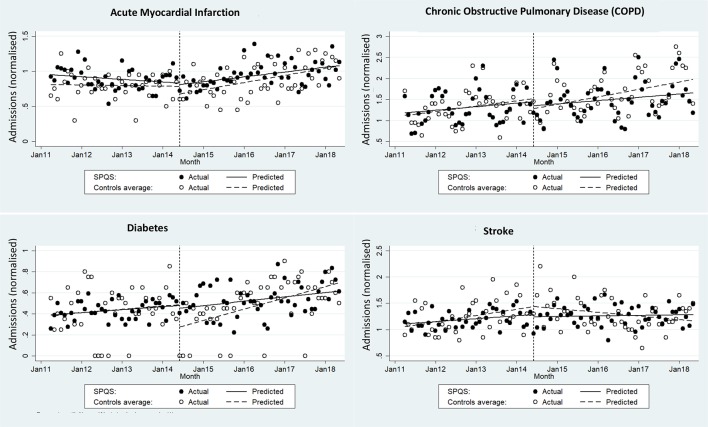
The evaluation used data from 55 SPQS practices and 17 regional control practices for three survey instruments. We collected patient experiences ('P3C-EQ'; 2363 returns from patients with 1+LTC; 36% response rate), staff experiences ('P3C-practitioner'; 127 professionals) and organisational data ('P3C-OCT'; 36 of 55 practices at two time points, 65% response rate; 17 control practices). Hospital Episode Statistics emergency admission data were analysed for 2014-2017 for ambulatory-sensitive conditions across Somerset using interrupted time series.
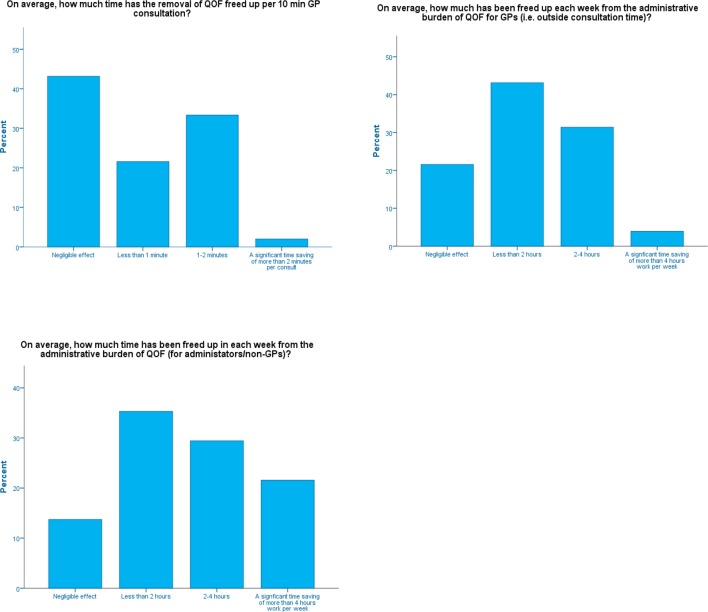
Patient and practitioner experiences were similar in SPQS versus control practices. However, discretion from QOF incentives resulted in time savings in the majority of practices, and SPQS practice data showed a significant increase in P3C oriented organisational processes, with a moderate effect size (Wilcoxon signed rank test; p=0.01; r=0.42). Analysis of transformation plans and organisational data suggested stronger federation-level agreements and informal networks, increased multidisciplinary working, reallocation of resources for other healthcare professionals and changes to the structure and timings of GP appointments. No disbenefits were detected in admission data.
The SPQS scheme leveraged time savings and reduced administrative burden via discretionary removal of QOF incentives, enabling practices to engage actively in a number of schemes aimed at improving care for people with LTCs. We found no differences in the experiences of patients or healthcare professionals between SPQS and control practices.
评估英国全科医生(GP)的质量和结果框架(QOF)奖励计划在全县范围内的去激励化。
2014 年,英国国民保健署(NHS England)表示,将 QOF 向临床委托小组(Clinical Commissioning Groups)下放。萨默塞特的 55 名全科医生设立了萨默塞特实践质量计划(SPQS)-QOF 的去激励措施-旨在将资源重新用于以人为本的协调护理(P3C),特别是针对患有长期疾病(LTCs)的患者。我们从 2016 年 4 月至 2017 年 3 月评估了对护理流程和结果的影响。
该评估使用了来自 55 个 SPQS 实践和 17 个区域控制实践的三个调查工具的数据。我们收集了患者体验('P3C-EQ';来自 1+LTC 患者的 2363 份回复;36%的回复率)、员工体验('P3C-从业者';127 名专业人员)和组织数据('P3C-OCT';在两个时间点上的 36 个 55 个实践中,65%的回复率;17 个对照实践)。对 2014 年至 2017 年萨默塞特的所有门诊敏感条件的医院入院统计数据进行了中断时间序列分析。
SPQS 与对照实践相比,患者和从业者的体验相似。然而,从 QOF 激励中获得的自由裁量权使大多数实践节省了时间,SPQS 实践数据显示 P3C 导向的组织流程显著增加,效果适中(Wilcoxon 符号秩检验;p=0.01;r=0.42)。转型计划和组织数据的分析表明,联邦一级的协议和非正式网络更加牢固,多学科工作增加,为其他医疗保健专业人员重新分配资源,以及 GP 预约的结构和时间发生变化。入院数据未发现不利影响。
SPQS 计划通过灵活运用去除 QOF 激励措施节省了时间并减轻了行政负担,使实践能够积极参与多项旨在改善长期疾病患者护理的计划。我们没有发现 SPQS 实践和对照实践在患者或医疗保健专业人员的体验上有差异。