Experimental and Clinical Research Center, Max Delbrueck Center for Molecular Medicine and Charité - Universitätsmedizin Berlin, Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Robert-Rössle-Straße 10, 13125, Berlin, Germany.
NeuroCure Clinical Research Center, Charité - Universitätsmedizin Berlin, Freie Universität Berlin, Humboldt-Universität zu Berlin and Berlin Institute of Health, Charitéplatz 1, 10117, Berlin, Germany.
J Neuroinflammation. 2019 Jul 25;16(1):154. doi: 10.1186/s12974-019-1521-5.
Serum antibodies against myelin-oligodendrocyte-glycoprotein (MOG-IgG) are detectable in a proportion of patients with acute or relapsing neuroinflammation. It is unclear, if neuro-axonal damage occurs only in an attack-dependent manner or also progressively. Therefore, this study aimed to investigate longitudinally intra-retinal layer changes in eyes without new optic neuritis (ON) in MOG-IgG-seropositive patients.
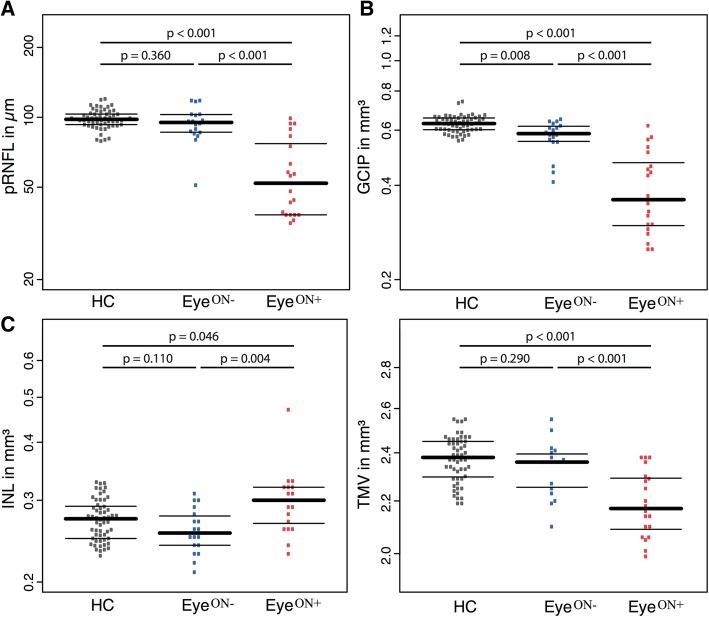
We included 38 eyes of 24 patients without ON during follow-up (F/U) [median years (IQR)] 1.9 (1.0-2.2) and 56 eyes of 28 age- and sex-matched healthy controls (HC). The patient group's eyes included 18 eyes without (Eye) and 20 eyes with history of ON (Eye). Using spectral domain optical coherence tomography (OCT), we acquired peripapillary retinal nerve fiber layer thickness (pRNFL) and volumes of combined ganglion cell and inner plexiform layer (GCIP), inner nuclear layer (INL), and macular volume (MV). High-contrast visual acuity (VA) was assessed at baseline.
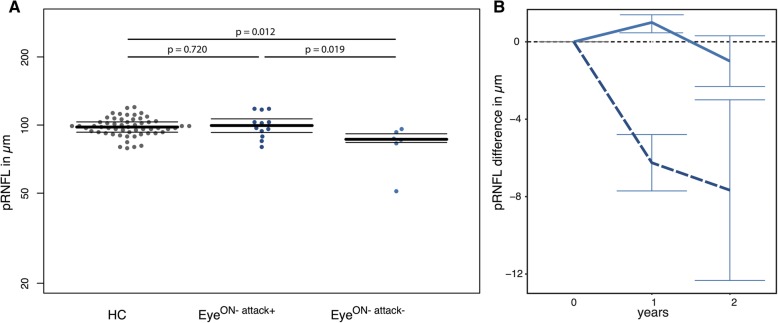
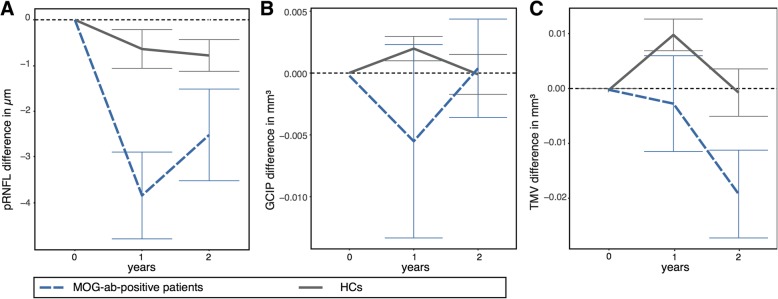
At baseline in Eye, pRNFL (94.3 ± 15.9 μm, p = 0.36), INL (0.26 ± 0.03 mm, p = 0.11), and MV (2.34 ± 0.11 mm, p = 0.29) were not reduced compared to HC; GCIP showed thinning (0.57 ± 0.07 mm; p = 0.008), and VA was reduced (logMAR 0.05 ± 0.15 vs. - 0.09 ± 0.14, p = 0.008) in comparison to HC. Longitudinally, we observed pRNFL thinning in models including all patient eyes (annual reduction - 2.20 ± 4.29 μm vs. - 0.35 ± 1.17 μm, p = 0.009) in comparison to HC. Twelve Eye with other than ipsilateral ON attacks ≤ 6 months before baseline showed thicker pRNFL at baseline and more severe pRNFL thinning in comparison to 6 Eye without other clinical relapses.
We observed pRNFL thinning in patients with MOG-IgG during F/U, which was not accompanied by progressive GCIP reduction. This effect could be caused by a small number of Eye with other than ipsilateral ON attacks within 6 months before baseline. One possible interpretation could be a reduction of the swelling, which could mean that MOG-IgG patients show immune-related swelling in the CNS also outside of an attack's target area.
髓鞘少突胶质细胞糖蛋白(MOG-IgG)血清抗体在一部分急性或复发的神经炎症患者中可被检测到。目前尚不清楚神经轴突损伤是否仅在发作依赖的情况下发生,还是也在进行性地发生。因此,本研究旨在纵向研究 MOG-IgG 阳性患者无新发视神经炎(ON)的眼内视网膜内各层的变化。
我们纳入了 24 例随访期间无 ON 的患者的 38 只眼[中位数(IQR)年数 1.9(1.0-2.2)]和 28 例年龄和性别匹配的健康对照者的 56 只眼。患者组的眼包括无 ON 史的 18 只眼(眼)和 20 只曾有 ON 史的眼(眼)。我们使用频域光学相干断层扫描(OCT)获得了视盘周围视网膜神经纤维层厚度(pRNFL)和联合神经节细胞和内丛状层(GCIP)、内核层(INL)和黄斑体积(MV)的体积。在基线时评估高对比度视力(VA)。
在眼的基线时,与 HC 相比,pRNFL(94.3 ± 15.9 μm,p = 0.36)、INL(0.26 ± 0.03 mm,p = 0.11)和 MV(2.34 ± 0.11 mm,p = 0.29)并未减少;GCIP 变薄(0.57 ± 0.07 mm,p = 0.008),VA 降低(logMAR 0.05 ± 0.15 与 -0.09 ± 0.14,p = 0.008),与 HC 相比。纵向研究中,与 HC 相比,我们观察到所有患者眼的模型中 pRNFL 变薄(每年减少 -2.20 ± 4.29 μm 与 -0.35 ± 1.17 μm,p = 0.009)。在基线前 6 个月内有同侧以外的 ON 发作≤6 次的 12 只眼基线时 pRNFL 较厚,pRNFL 变薄更严重。
我们在 MOG-IgG 患者的随访中观察到 pRNFL 变薄,而 GCIP 没有进行性减少。这种影响可能是由于在基线前 6 个月内有少数眼发生了同侧以外的 ON 发作。一种可能的解释是肿胀减轻,这意味着 MOG-IgG 患者在发作靶区以外的中枢神经系统中也表现出与免疫相关的肿胀。