From the Moorfields Eye Hospital NHS Foundation Trust (G.V., N.J., G.G.), London, United Kingdom; Department of Ophthalmology (G.V.), Institute of Clinical Neurosciences of Southern Switzerland (INSI), Ente Ospedaliero Cantonale (EOC), Lugano, Switzerland; Department of Neuro-ophthalmology (N.J.), The National Hospital for Neurology and Neurosurgery, UCL Queen Square Institute of Neurology, The National Hospital for Neurology and Neurosurgery; Institute of Ophthalmology (N.J.), University College London, United Kingdom; Federal University of the State of Rio de Janeiro (UNIRIO) (G.G.), Brazil; Einstein Center for Digital Future Berlin (H.G.Z.); Experimental and Clinical Research Center (ECRC) (H.G.Z., S.M., C.B., A.U.B., F.P., F.C.O.), Max-Delbrueck-Center Berlin & Charité - Universitätsmedizin Berlin; Neuroscience Clinical Research Center (NCRC) (H.G.Z., S.M., C.B., A.U.B., F.P., F.C.O.), Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Germany; Centre for Advanced Neurological Research (L.P., A.D.C.), Nitte University, Mangalore, India; Department of Medicine (M.R.Y.), David Geffen School of Medicine at UCLA, Los Angeles; Divisions of Molecular Medicine and Infectious Diseases (M.R.Y.), Department of Medicine; Lundquist Institute for Biomedical Innovation at Harbor-University of California Los Angeles Medical Center (M.R.Y.), Torrance, CA; Departments of Ophthalmology and Visual Sciences (T.J.S.), Kellogg Eye Center; Division of Metabolism (T.J.S.), Endocrine and Diabetes, Department of Internal Medicine, University of Michigan Medical School, Ann Arbor; Department of Pediatrics (L.J.C.), University of Utah; Department of Neurology (F.P., F.C.O.), Charité - Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Germany; National Hospital for Neurology and Neurosurgery (A.P.), University College London Hospitals NHS Foundation Trust, Moorfields Eye Hospital NHS Foundation Trust and Queen Square Dept. of Neuroinflammation, UCL, Queen Square Institute of Neurology, University College London, United Kingdom; and Neuro-ophthalmology Expert Centre (A.P.), Amsterdam University Medical Center, The Netherlands.
Neurol Neuroimmunol Neuroinflamm. 2024 Nov;11(6):e200291. doi: 10.1212/NXI.0000000000200291. Epub 2024 Sep 4.
The 2022 International Consortium for Optic Neuritis diagnostic criteria for optic neuritis (ON) include optical coherence tomography (OCT). The diagnostic value of intereye difference (IED) metrics is high for ON in patients with multiple sclerosis and aquaporin-4 antibody seropositive neuromyelitis optica spectrum disorders, but unknown in myelin oligodendrocyte glycoprotein antibody-associated ON (MOG-ON).
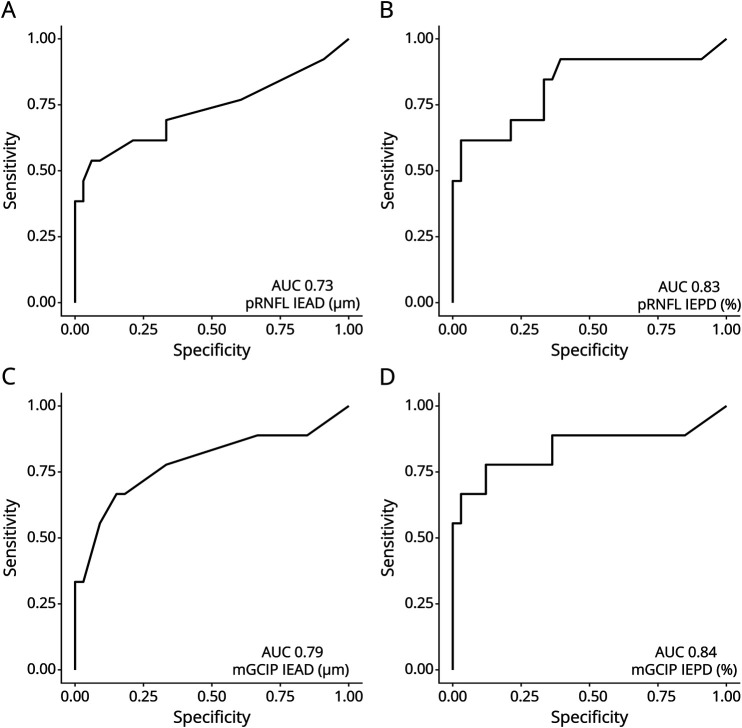
A multicenter validation study was conducted on the published IED cutoff values (>4% or >4 μm in the macular ganglion cell and inner plexiform layer [mGCIP] or >5% or >5 μm in the peripapillary retinal nerve fiber layer [pRNFL]) in individuals with MOG-ON and age-matched and sex-matched healthy controls (HCs). Structural data were acquired with Spectralis spectral-domain OCT >6 months after ON. We calculated sensitivity, specificity, and receiver operating characteristics for both intereye percentage (IEPD) and absolute difference (IEAD).
A total of 66 individuals were included (MOG-ON N = 33; HCs N = 33). ON was unilateral in 20 and bilateral in 13 subjects. In the pooled analysis, the mGCIP IEPD was most sensitive (92%), followed by the mGCIP IEAD (88%) and pRNFL (84%). The same pattern was found for the specificity (mGCIP IEPD 82%, IEAD 82%; pRNFL IEPD 82%, IEAD 79%).In subgroup analyses, the diagnostic sensitivity was higher in subjects with unilateral ON (>99% for all metrics) compared with bilateral ON (61%-78%).
In individuals with MOG-ON, the diagnostic accuracy of OCT-based IED metrics for ON was high, especially of mGCIP IEPD.
This study provides Class III evidence that the intereye difference on OCT can distinguish between those with MOG and normal controls.
2022 年视神经炎国际联合会诊断标准(ON)包括光学相干断层扫描(OCT)。在多发性硬化症和水通道蛋白 4 抗体阳性视神经脊髓炎谱系障碍患者中,双眼间差异(IED)指标对 ON 的诊断价值较高,但在髓鞘少突胶质细胞糖蛋白抗体相关性 ON(MOG-ON)中尚不清楚。
对已发表的 MOG-ON 患者和年龄、性别匹配的健康对照者(HCs)中 IED 截断值(黄斑神经节细胞和内丛状层[macular ganglion cell and inner plexiform layer,mGCIP]>4%或>4μm,或视盘周围视网膜神经纤维层[peripapillary retinal nerve fiber layer,pRNFL] >5%或>5μm)进行多中心验证研究。ON 后 6 个月以上采用 Spectralis 光谱域 OCT 采集结构数据。我们计算了双眼间百分比(IEPD)和绝对差值(IEAD)的敏感性、特异性和受试者工作特征。
共纳入 66 例患者(MOG-ON 33 例;HCs 33 例)。20 例为单侧 ON,13 例为双侧 ON。在汇总分析中,mGCIP IEPD 最敏感(92%),其次是 mGCIP IEAD(88%)和 pRNFL(84%)。特异性也呈现相同模式(mGCIP IEPD 82%,IEAD 82%;pRNFL IEPD 82%,IEAD 79%)。在亚组分析中,单侧 ON 患者的诊断敏感性较高(所有指标均>99%),而双侧 ON 患者的诊断敏感性为 61%-78%。
在 MOG-ON 患者中,基于 OCT 的 IED 指标对 ON 的诊断准确性较高,尤其是 mGCIP IEPD。
本研究提供 III 级证据,表明 OCT 上的双眼间差异可区分 MOG 与正常对照者。