Paschalis Alec, Sheehan Beshara, Riisnaes Ruth, Rodrigues Daniel Nava, Gurel Bora, Bertan Claudia, Ferreira Ana, Lambros Maryou B K, Seed George, Yuan Wei, Dolling David, Welti Jon C, Neeb Antje, Sumanasuriya Semini, Rescigno Pasquale, Bianchini Diletta, Tunariu Nina, Carreira Suzanne, Sharp Adam, Oyen Wim, de Bono Johann S
The Institute of Cancer Research, Sutton, UK; The Royal Marsden NHS Foundation Trust, Sutton, UK.
The Institute of Cancer Research, Sutton, UK.
Eur Urol. 2019 Oct;76(4):469-478. doi: 10.1016/j.eururo.2019.06.030. Epub 2019 Jul 22.
Prostate-specific membrane antigen (PSMA; folate hydrolase) prostate cancer (PC) expression has theranostic utility.
To elucidate PC PSMA expression and associate this with defective DNA damage repair (DDR).
DESIGN, SETTING, AND PARTICIPANTS: Membranous PSMA (mPSMA) expression was scored immunohistochemically from metastatic castration-resistant PC (mCRPC) and matching, same-patient, diagnostic biopsies, and correlated with next-generation sequencing (NGS) and clinical outcome data.
Expression of mPSMA was quantitated by modified H-score. Patient DNA was tested by NGS. Gene expression and activity scores were determined from mCRPC transcriptomes. Statistical correlations utilised Wilcoxon signed rank tests, survival was estimated by Kaplan-Meier test, and sample heterogeneity was quantified by Shannon's diversity index.
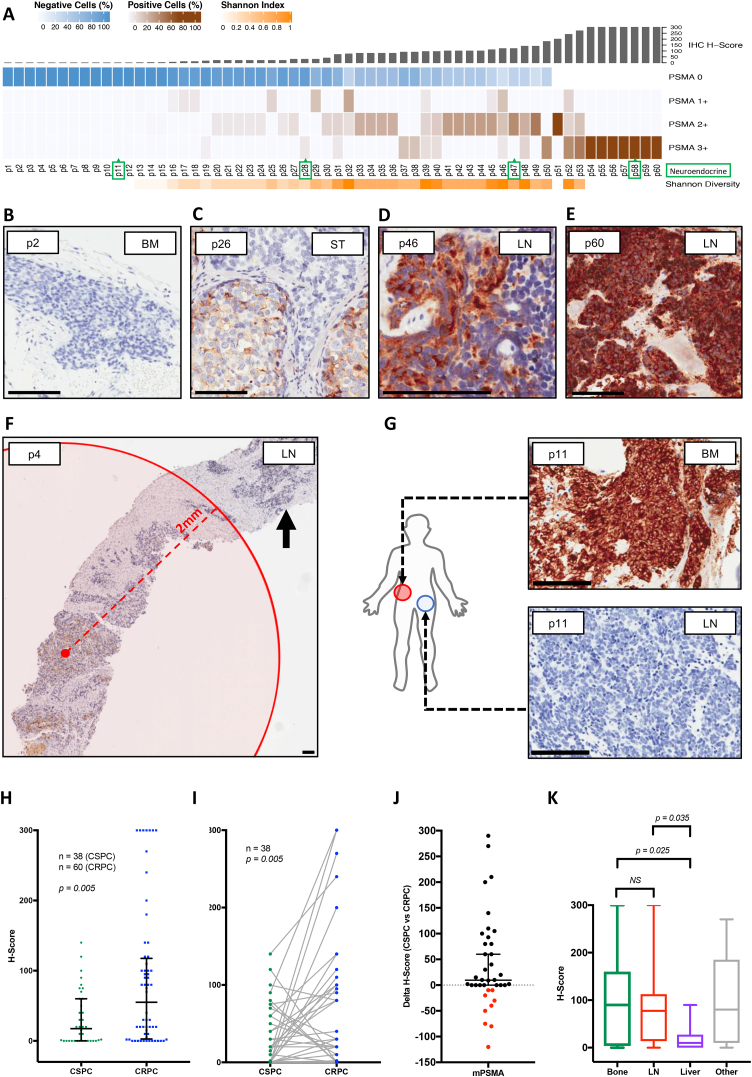
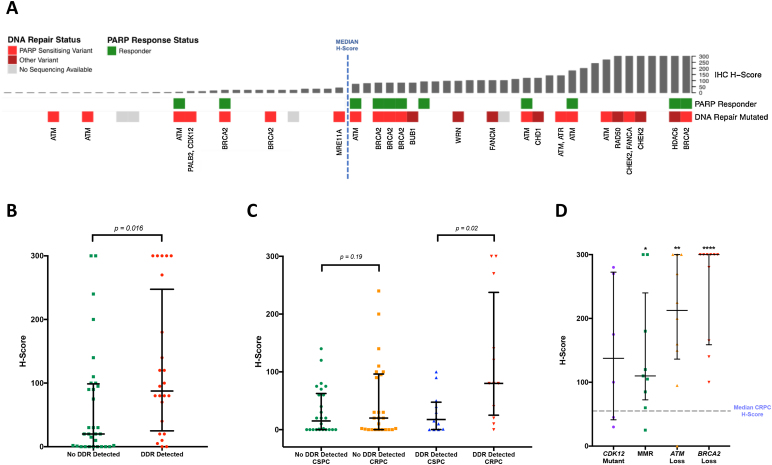
Expression of mPSMA at diagnosis was associated with higher Gleason grade (p=0.04) and worse overall survival (p=0.006). Overall, mPSMA expression levels increased at mCRPC (median H-score [interquartile range]: castration-sensitive prostate cancer [CSPC] 17.5 [0.0-60.0] vs mCRPC 55.0 [2.8-117.5]). Surprisingly, 42% (n=16) of CSPC and 27% (n=16) of mCRPC tissues sampled had no detectable mPSMA (H-score <10). Marked intratumour heterogeneity of mPSMA expression, with foci containing no detectable PSMA, was observed in all mPSMA expressing CSPC (100%) and 37 (84%) mCRPC biopsies. Heterogeneous intrapatient mPSMA expression between metastases was also observed, with the lowest expression in liver metastases. Tumours with DDR had higher mPSMA expression (p=0.016; 87.5 [25.0-247.5] vs 20 [0.3-98.8]; difference in medians 60 [5.0-95.0]); validation cohort studies confirmed higher mPSMA expression in patients with deleterious aberrations in BRCA2 (p<0.001; median H-score: 300 [165-300]; difference in medians 195.0 [100.0-270.0]) and ATM (p=0.005; 212.5 [136.3-300]; difference in medians 140.0 [55.0-200]) than in molecularly unselected mCRPC biopsies (55.0 [2.75-117.5]). Validation studies using mCRPC transcriptomes corroborated these findings, also indicating that SOX2 high tumours have low PSMA expression.
Membranous PSMA expression is upregulated in some but not all PCs, with mPSMA expression demonstrating marked inter- and intrapatient heterogeneity. DDR aberrations are associated with higher mPSMA expression and merit further evaluation as predictive biomarkers of response for PSMA-targeted therapies in larger, prospective cohorts.
Through analysis of prostate cancer samples, we report that the presence of prostate-specific membrane antigen (PSMA) is extremely variable both within one patient and between different patients. This may limit the usefulness of PSMA scans and PSMA-targeted therapies. We show for the first time that prostate cancers with defective DNA repair produce more PSMA and so may respond better to PSMA-targeting treatments.
前列腺特异性膜抗原(PSMA;叶酸水解酶)在前列腺癌(PC)中的表达具有诊疗效用。
阐明PC中PSMA的表达情况,并将其与DNA损伤修复缺陷(DDR)相关联。
设计、设置和参与者:通过免疫组织化学对转移性去势抵抗性PC(mCRPC)以及匹配的同一患者诊断性活检组织中的膜性PSMA(mPSMA)表达进行评分,并与二代测序(NGS)和临床结局数据相关联。
通过改良H评分对mPSMA的表达进行定量。患者DNA通过NGS进行检测。从mCRPC转录组中确定基因表达和活性评分。统计相关性采用Wilcoxon符号秩检验,生存情况通过Kaplan-Meier检验进行估计,样本异质性通过香农多样性指数进行量化。
诊断时mPSMA的表达与更高的Gleason分级相关(p=0.04),且总生存期更差(p=0.006)。总体而言,mCRPC时mPSMA表达水平升高(中位数H评分[四分位间距]:去势敏感性前列腺癌[CSPC]为17.5[0.0-60.0],而mCRPC为55.0[2.8-117.5])。令人惊讶的是,42%(n=16)的CSPC组织样本和27%(n=16)的mCRPC组织样本未检测到可检测的mPSMA(H评分<10)。在所有表达mPSMA的CSPC(100%)和所有37例(84%)mCRPC活检组织中均观察到mPSMA表达存在明显的肿瘤内异质性,存在未检测到PSMA的病灶。在转移灶之间也观察到患者体内mPSMA表达存在异质性,肝转移灶中表达最低。存在DDR的肿瘤mPSMA表达更高(p=0.016;87.5[25.0-247.5]对比20[0.3-98.8];中位数差异为60[5.0-95.0]);验证队列研究证实,与分子未筛选的mCRPC活检组织(55.0[2.75-117.5])相比,BRCA2(p<0.001;中位数H评分:300[165-300];中位数差异为195.0[100.0-270.0])和ATM(p=0.005;212.5[136.3-300];中位数差异为140.0[55.0-200])存在有害畸变的患者mPSMA表达更高。使用mCRPC转录组的验证研究证实了这些发现,还表明SOX2高表达的肿瘤PSMA表达较低。
膜性PSMA表达在部分而非所有PC中上调,mPSMA表达表现出明显的患者间和患者内异质性。DDR畸变与更高的mPSMA表达相关,在更大规模的前瞻性队列中作为PSMA靶向治疗反应的预测生物标志物值得进一步评估。
通过对前列腺癌样本的分析,我们报告前列腺特异性膜抗原(PSMA)的存在在同一患者体内以及不同患者之间差异极大。这可能会限制PSMA扫描和PSMA靶向治疗的效用。我们首次表明,DNA修复存在缺陷的前列腺癌产生更多的PSMA,因此可能对PSMA靶向治疗反应更好。