1Advanced Critical Care and Emergency Center, Yokohama City University Medical Center, 4-57 Urafunecho, Minami-ku, Yokohama, Kanagawa 232-0024 Japan.
2Department of Emergency Medicine, Graduate School of Medicine, Yokohama City University, 3-9 Fukuura, Kanazawa-ku, Yokohama, Kanagawa 236-0004 Japan.
World J Emerg Surg. 2019 Jul 16;14:35. doi: 10.1186/s13017-019-0255-0. eCollection 2019.
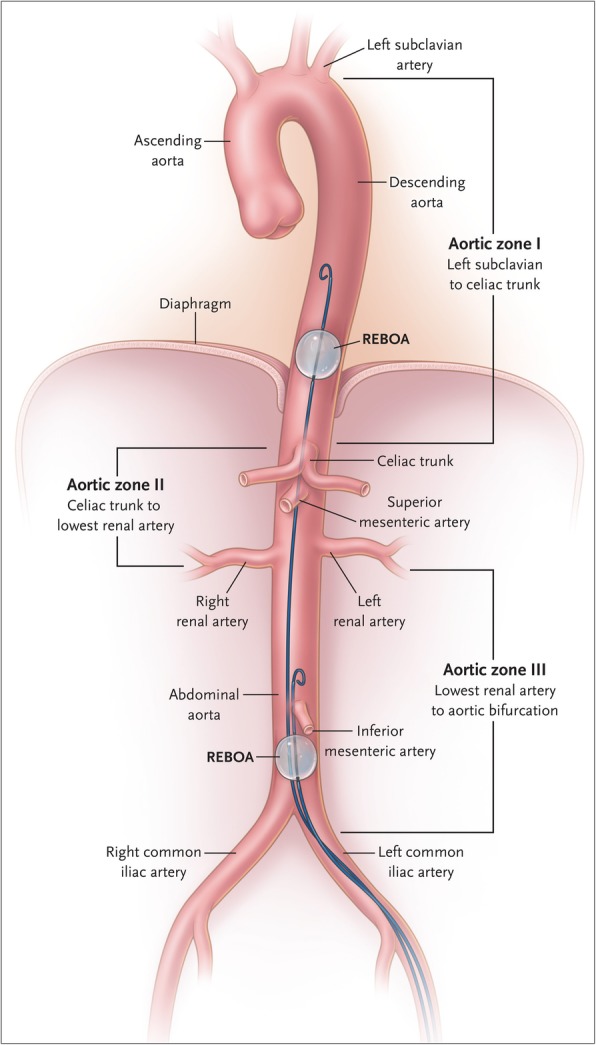
Resuscitative endovascular balloon occlusion of the aorta (REBOA) for patients with traumatic torso hemorrhagic shock is available to keep a minimum level of circulatory status as a bridge to definitive therapy. However, the trajectory for placement of REBOA in the aorta has not yet been clearly defined.
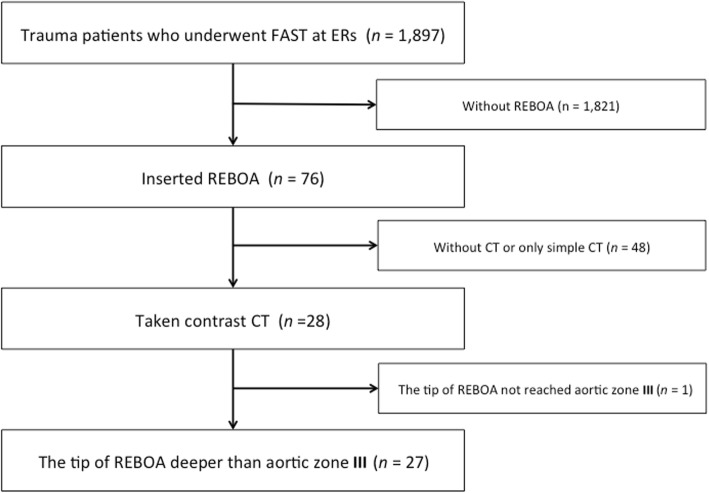
We conducted a retrospective observational cohort study in the two tertiary critical care and emergency center from December 2014 to October 2018. A total of 28 patients who underwent focused assessment with sonography for trauma (FAST) were studied via contrast computed tomography (CT), and 27 were analyzed.
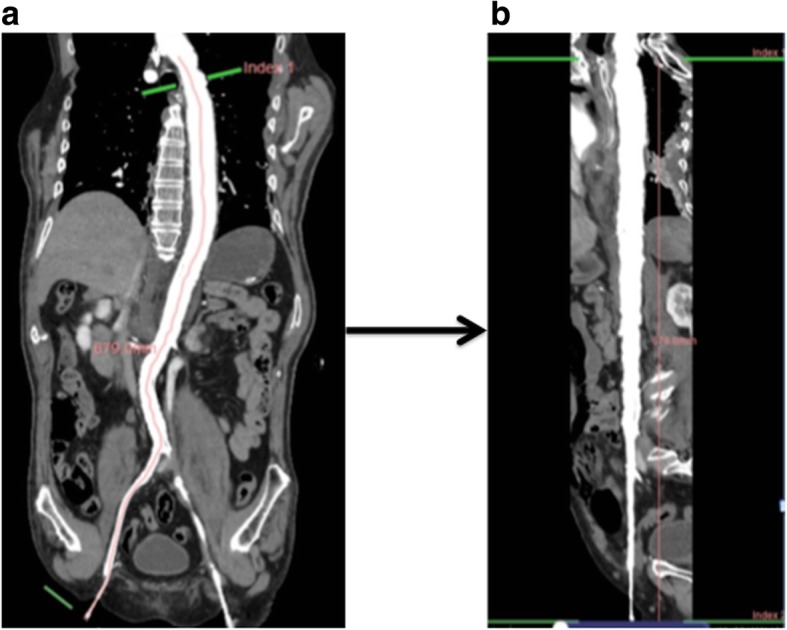
We divided patients into two groups based on our CT findings. The REBOA deflate group included 16 patients, and the inflate group included 11 patients. The median trace value (interquartile range) of the blood vessel center line from the common femoral artery to the tip of REBOA (blood vessel length) and the length of REBOA itself from the common femoral artery to the tip of REBOA (REBOA insertion length) were 56.2 cm (54.5-57.2) and 55.2 cm (54.2-55.6), respectively ( < 0.0001) for the deflated group, and 51.4 cm (42.1-56.6) and 50.3 cm (42.3-55.0) ( = 0.594), respectively, for the inflated group.
If REBOA was deflated, it was placed 1.0 cm longer than the insertion length of REBOA catheter itself, but that was not the case when inflating REBOA. The individual difference was large to the extent that the balloon inflated and the extent to which the balloon was pushed back toward the caudal depending on the degree of blood pressure. Further studies would be needed to validate the study findings.
主动脉球囊阻断复苏术(REBOA)用于创伤性躯干出血性休克患者,可保持最低循环状态,作为确定性治疗的桥梁。然而,主动脉内 REBOA 的放置轨迹尚未明确界定。
我们对 2014 年 12 月至 2018 年 10 月期间在两个三级重症监护和急救中心进行了一项回顾性观察队列研究。对 28 例接受创伤超声重点评估(FAST)的患者进行了对比 CT 检查,其中 27 例进行了分析。
根据我们的 CT 结果,我们将患者分为两组。REBOA 放气组包括 16 例患者,充气组包括 11 例患者。从股总动脉到 REBOA 尖端的血管中心线(血管长度)和从股总动脉到 REBOA 尖端的 REBOA 自身长度(REBOA 插入长度)的中位数(四分位间距)分别为 56.2cm(54.5-57.2)和 55.2cm(54.2-55.6)( < 0.0001),对于放气组,分别为 51.4cm(42.1-56.6)和 50.3cm(42.3-55.0)( = 0.594),分别为充气组。
如果 REBOA 放气,它比 REBOA 导管自身插入长度长 1.0cm,但充气时并非如此。个体差异很大,程度取决于血压,气囊充气和气囊向尾部回推的程度。需要进一步的研究来验证研究结果。