Zhang Shenqi, Wang Chengbin, Shi Lei, Xue Qingyun
Department of Orthopedics, Beijing Hospital ,National Center of Gerontology, PR China.
Graduate School of Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing.
Medicine (Baltimore). 2019 Jul;98(30):e16570. doi: 10.1097/MD.0000000000016570.
Perioperative bleeding during total knee arthroplasty (TKA) is an ongoing problem for surgeons. Intravenous or topical application of tranexamic acid (TXA) can effectively stop bleeding, but there is still no uniform standard for the best method of administration and dose.
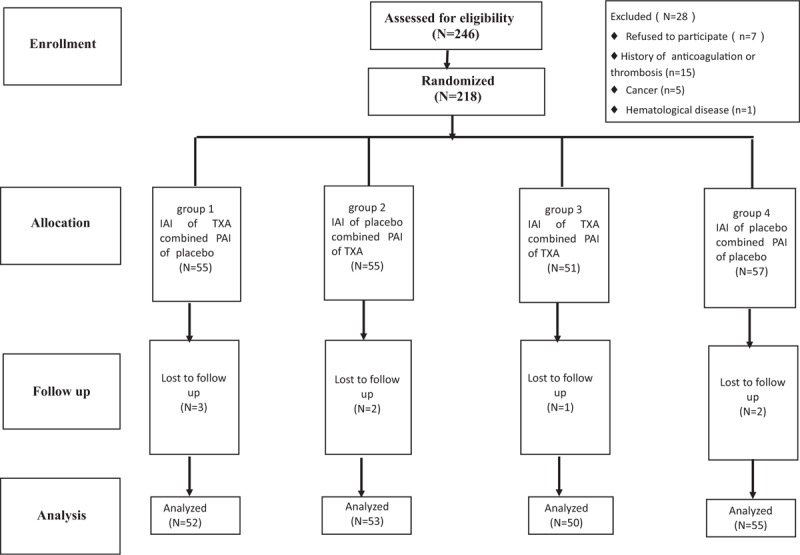
From October 2016 to September 2018, 218 patients with unilateral primary knee osteoarthritis requiring knee replacement were enrolled and randomly divided into four groups. Group 1 (n = 55) received intra-articular injection (IAI) of TXA and peri-articular injection (PAI) of placebo, group 2 (n = 55) received IAI of placebo and PAI of TXA, group 3 (n = 51) received IAI of TXA and PAI of TXA, and group 4 (n = 57) received double placebo (IAI of placebo and PAI of placebo). The demographic characteristics, surgical indices, hematological indices, wound healing history, and thromboembolic events were investigated.
Eight patients were lost to follow-up and 210 patients were included in the analysis. The median TBLs in patients who received IAI of TXA and PAI of placebo and those who received IAI of placebo and PAI of TXA were 470.81 ml and 481.54 ml, respectively. These TBL levels were significantly higher compared to those in patients who received IAI of TXA and PAI of TXA (359.18 ml, P ≤ .001), but significantly lower compared to those in patients who received the double placebo (522.71 ml, P ≤ .001). Compared to other groups, more patients in the double placebo group needed a blood transfusion (P = .013). In the short-term, the double placebo group had higher VAS pain scores and less ROM after surgery (P = .011 and P = .001, respectively). In the long-term (6-month follow-up), there were no significant differences in ROM, VAS, DVT, PE, or wound-related complications.
The combined use of IAI and PAI of TXA can significantly reduce the TBL and the need for blood transfusion without delaying wound healing or increasing the risk of DVT and PE. In the short-term after surgery, this combined method reduces the pain VAS scores and improves the ROM; however, there are no long-term effects on VAS and ROM.
全膝关节置换术(TKA)围手术期出血一直是外科医生面临的问题。静脉注射或局部应用氨甲环酸(TXA)可有效止血,但最佳给药方法和剂量仍没有统一标准。
2016年10月至2018年9月,纳入218例需要行膝关节置换术的单侧原发性膝关节骨关节炎患者,并随机分为四组。第1组(n = 55)接受关节内注射(IAI)TXA和关节周围注射(PAI)安慰剂,第2组(n = 55)接受IAI安慰剂和PAI TXA,第3组(n = 51)接受IAI TXA和PAI TXA,第4组(n = 57)接受双安慰剂(IAI安慰剂和PAI安慰剂)。调查患者的人口统计学特征、手术指标、血液学指标、伤口愈合情况及血栓栓塞事件。
8例患者失访,210例患者纳入分析。接受IAI TXA和PAI安慰剂的患者以及接受IAI安慰剂和PAI TXA的患者的中位失血量分别为470.81 ml和481.54 ml。与接受IAI TXA和PAI TXA的患者(359.18 ml,P≤0.001)相比,这些失血量水平显著更高,但与接受双安慰剂的患者(522.71 ml,P≤0.001)相比显著更低。与其他组相比,双安慰剂组更多患者需要输血(P = 0.013)。短期内,双安慰剂组术后视觉模拟评分(VAS)疼痛评分更高,关节活动度(ROM)更小(分别为P = 0.011和P = 0.001)。长期(6个月随访)时,ROM、VAS、深静脉血栓形成(DVT)、肺栓塞(PE)或伤口相关并发症方面无显著差异。
TXA的IAI和PAI联合使用可显著减少失血量和输血需求,且不延迟伤口愈合或增加DVT和PE风险。术后短期内,这种联合方法可降低VAS疼痛评分并改善ROM;然而,对VAS和ROM无长期影响。