Division of Cardiovascular Surgery, Department of Surgery, University of Pennsylvania, Philadelphia, Pa; Department of Bioengineering, University of Pennsylvania, Philadelphia, Pa.
Division of Cardiovascular Surgery, Department of Surgery, University of Pennsylvania, Philadelphia, Pa; Department of Bioengineering, University of Pennsylvania, Philadelphia, Pa.
J Thorac Cardiovasc Surg. 2020 May;159(5):1825-1835.e2. doi: 10.1016/j.jtcvs.2019.06.017. Epub 2019 Jun 18.
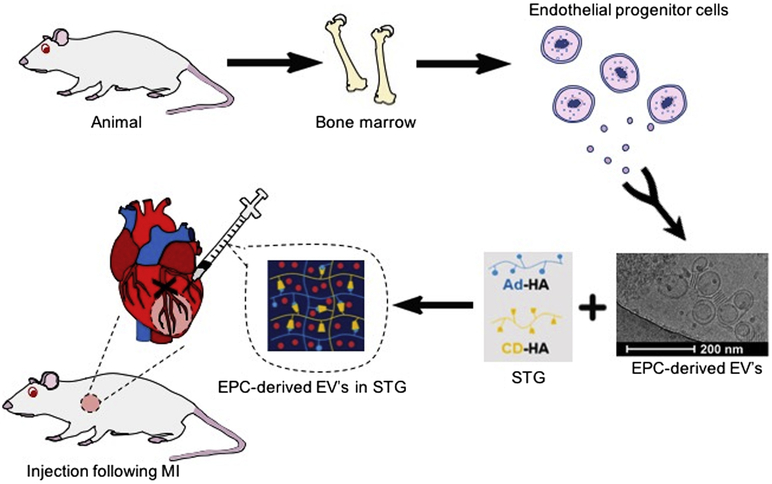
Extracellular vesicles (EVs) are promising therapeutics for cardiovascular disease, but poorly-timed delivery might hinder efficacy. We characterized the time-dependent response to endothelial progenitor cell (EPC)-EVs within an injectable shear-thinning hydrogel (STG+EV) post-myocardial infarction (MI) to identify when an optimal response is achieved.
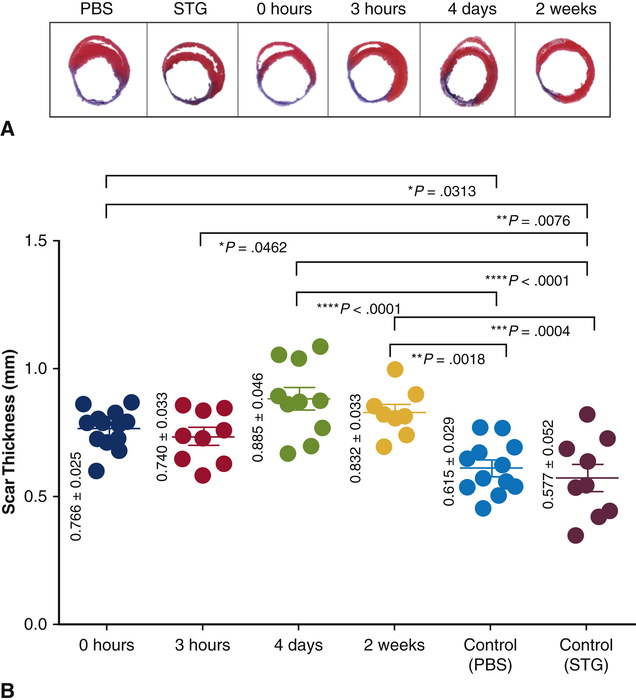
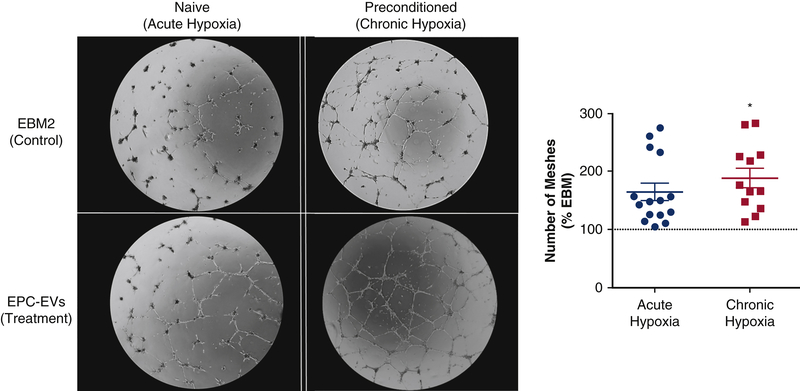
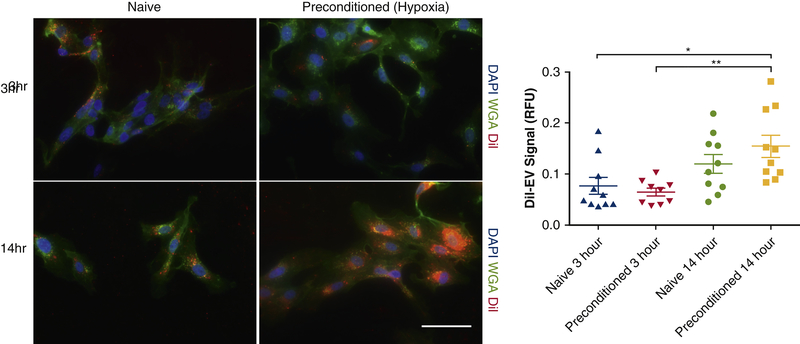
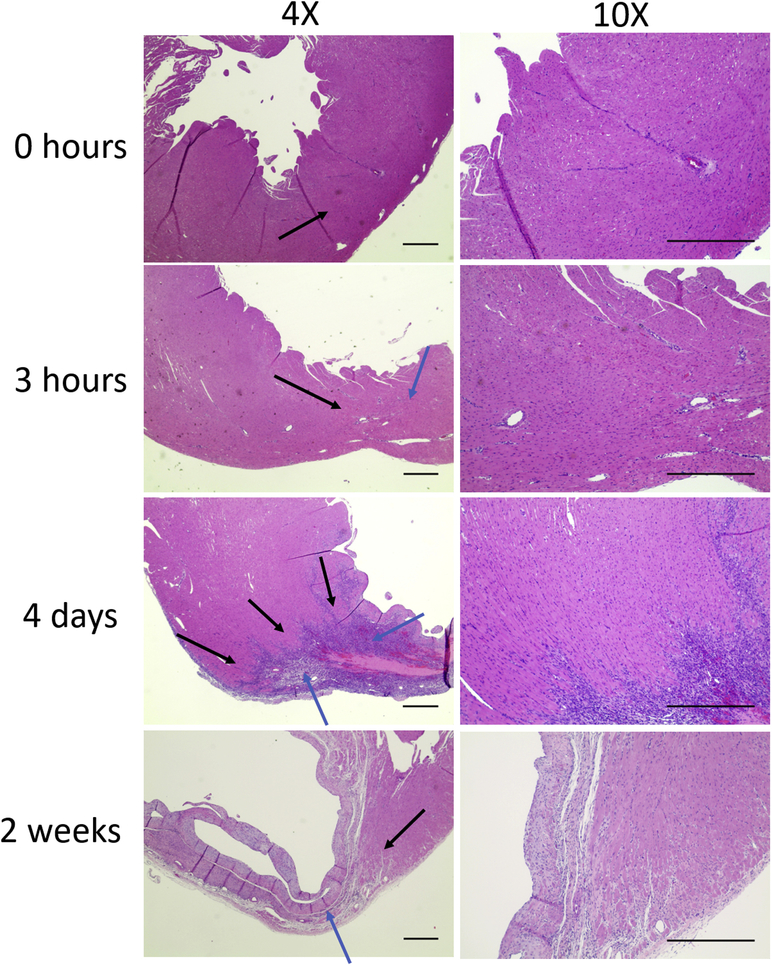
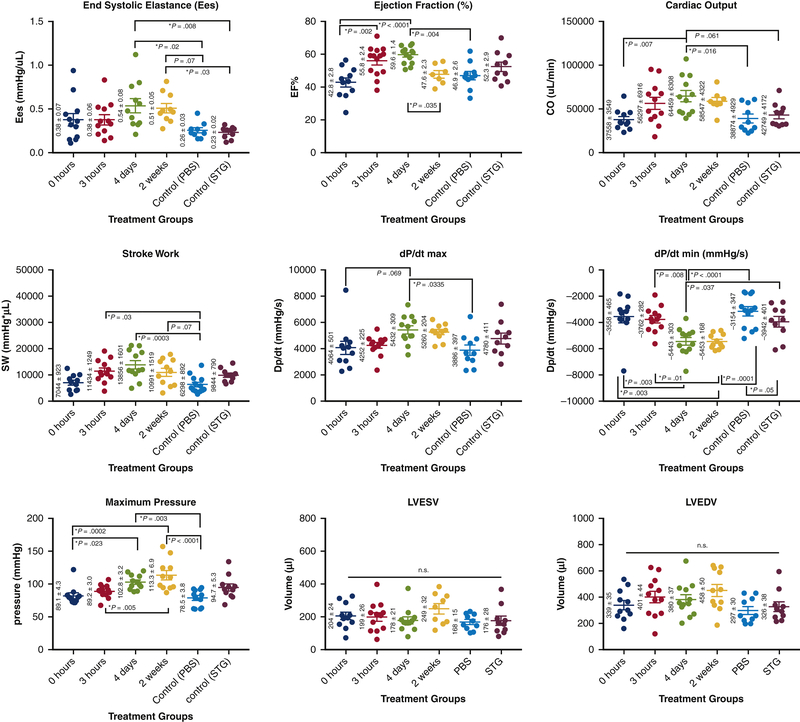
The angiogenic effects of prolonged hypoxia on cell response to EPC-EV therapy and EV uptake affinity were tested in vitro. A rat model of acute MI via left anterior descending artery ligation was created and STG+EV was delivered via intramyocardial injections into the infarct border zone at time points corresponding to phases of post-MI inflammation: 0 hours (immediate), 3 hours (acute inflammation), 4 days (proliferative), and 2 weeks (fibrosis). Hemodynamics 4 weeks post-treatment were compared across treatment and control groups (phosphate buffered saline [PBS], shear-thinning gel). Scar thickness and ventricular diameter were assessed histologically. The primary hemodynamic end point was end systolic elastance. The secondary end point was scar thickness.
EPC-EVs incubated with chronically versus acutely hypoxic human umbilical vein endothelial cells resulted in a 2.56 ± 0.53 versus 1.65 ± 0.15-fold increase (P = .05) in a number of vascular meshes and higher uptake of EVs over 14 hours. End systolic elastance improved with STG+EV therapy at 4 days (0.54 ± 0.08) versus PBS or shear-thinning gel (0.26 ± 0.03 [P = .02]; 0.23 ± 0.02 [P = .01]). Preservation of ventricular diameter (6.20 ± 0.73 mm vs 8.58 ± 0.38 mm [P = .04]; 9.13 ± 0.25 mm [P = .01]) and scar thickness (0.89 ± 0.05 mm vs 0.62 ± 0.03 mm [P < .0001] and 0.58 ± 0.05 mm [P < .0001]) was significantly greater at 4 days, compared wit PBS and shear-thinning gel controls.
Delivery of STG+EV 4 days post-MI improved left ventricular contractility and preserved global ventricular geometry, compared with controls and immediate therapy post-MI. These findings suggest other cell-derived therapies can be optimized by strategic timing of therapeutic intervention.
细胞外囊泡(EVs)是心血管疾病有前途的治疗方法,但时机不佳可能会阻碍疗效。我们在心肌梗死后(MI)内,对可注射剪切稀化水凝胶(STG+EV)中内皮祖细胞(EPC)-EV 的时间依赖性反应进行了特征描述,以确定何时能达到最佳反应。
在体外测试了延长缺氧对细胞对 EPC-EV 治疗反应和 EV 摄取亲和力的影响。通过左前降支结扎建立大鼠急性 MI 模型,并在 MI 后炎症的各个阶段(0 小时[即刻]、3 小时[急性炎症]、4 天[增殖]和 2 周[纤维化])通过心肌内注射将 STG+EV 递送至梗死边界区。比较治疗组和对照组(磷酸盐缓冲盐水[PBS]、剪切稀化凝胶)治疗后 4 周的血流动力学。组织学评估瘢痕厚度和心室直径。主要血流动力学终点为收缩末期弹性。次要终点为瘢痕厚度。
与急性低氧相比,慢性低氧培养的 EPC-EVs 导致血管网格数量增加 2.56 ± 0.53 倍,14 小时内 EV 摄取增加 1.65 ± 0.15 倍。STG+EV 治疗在 4 天时改善了收缩末期弹性(0.54 ± 0.08)与 PBS 或剪切稀化凝胶(0.26 ± 0.03[P=0.02];0.23 ± 0.02[P=0.01])。与 PBS 和剪切稀化凝胶对照组相比,4 天时心室直径(6.20 ± 0.73 mm 比 8.58 ± 0.38 mm[P=0.04];9.13 ± 0.25 mm[P=0.01])和瘢痕厚度(0.89 ± 0.05 mm 比 0.62 ± 0.03 mm[P<0.0001]和 0.58 ± 0.05 mm[P<0.0001])的保存效果更好。
与 MI 后即刻治疗和对照组相比,MI 后 4 天递送 STG+EV 可改善左心室收缩功能并维持整体心室几何形状。这些发现表明,其他细胞衍生疗法可以通过治疗干预的策略性时机优化。