Department of Neurosurgery, OLVG and Amsterdam University Medical Centers, Amsterdam, the Netherlands.
Section for Spine Surgery, Klinikum Itzehoe, Itzehoe, Germany.
Clin Interv Aging. 2019 Jun 19;14:1085-1094. doi: 10.2147/CIA.S208098. eCollection 2019.
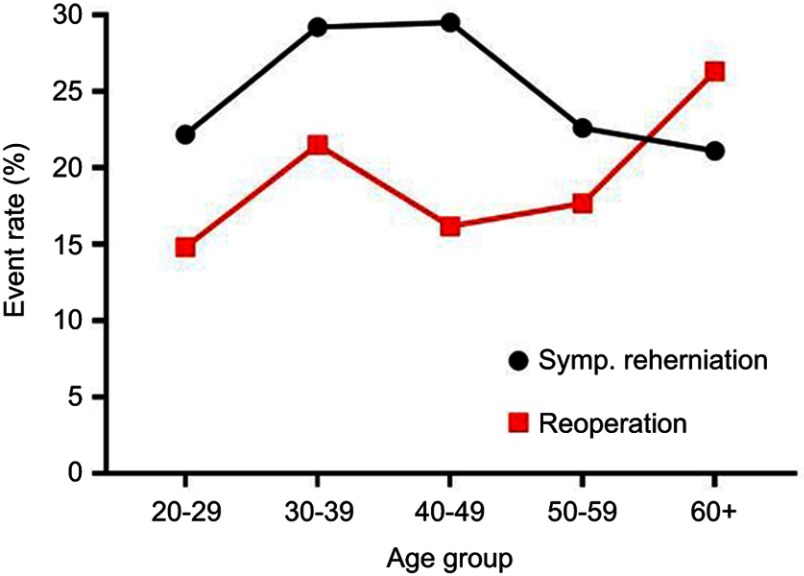
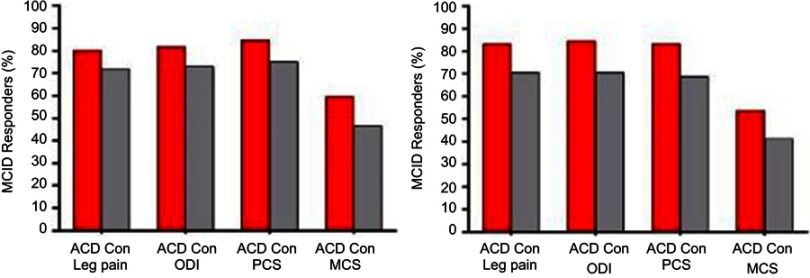
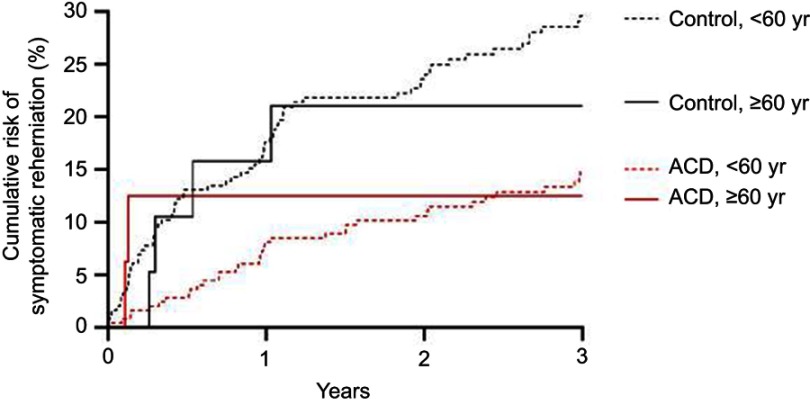
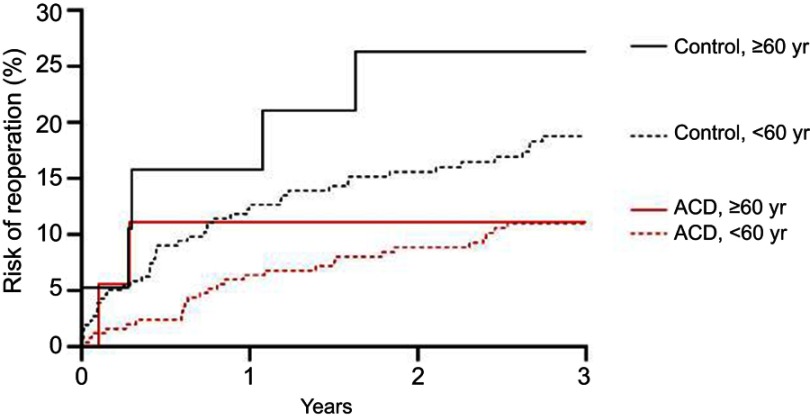
Lumbar discectomy is a common surgical procedure in middle-aged adults. However, outcomes of lumbar discectomy among older adults are unclear. Lumbar discectomy patients with an annular defect ≥6 mm width were randomized to receive additional implantation with a bone-anchored annular closure device (ACD, n=272) or no additional implantation (controls, n=278). Over 3 years follow-up, main outcomes were symptomatic reherniation, reoperation, and the percentage of patients who achieved the minimum clinically important difference (MCID) without a reoperation for leg pain, Oswestry Disability Index (ODI), SF-36 Physical Component Summary (PCS) score, and SF-36 Mental Component Summary (MCS) score. Results were compared between older (≥60 years) and younger (<60 years) patients. We additionally analyzed data from two postmarket ACD registries to determine consistency of outcomes between the randomized trial and postmarket, real-world results. Among all patients, older patients suffered from crippling or bed-bound preoperative disability more frequently than younger patients (57.9% vs 39.1%, =0.03). Among controls, female sex, higher preoperative ODI, and current smoking status, but not age, were associated with greater risk of reherniation and reoperation. Compared to controls, the ACD group had lower risk of symptomatic reherniation (HR=0.45, <0.001) and reoperation (HR=0.54, =0.008), with risk reductions comparable in older vs younger patients. The percentage of patients achieving the MCID without a reoperation was higher in the ACD group for leg pain (81% vs 72%, =0.04), ODI (82% vs 73%, =0.03), PCS (85% vs 75%, =0.01), and MCS (59% vs 46%, =0.007), and this benefit was comparable in older versus younger patients. Comparable benefits in older patients were observed in the postmarket ACD registries. Outcomes with lumbar discectomy and additional bone-anchored ACD are superior to lumbar discectomy alone. Older patients derived similar benefits with additional bone-anchored ACD implantation as younger patients.
腰椎间盘切除术是中年成年人常见的手术。然而,老年人腰椎间盘切除术的结果尚不清楚。对于环形缺陷≥6 毫米的腰椎间盘切除术患者,随机分为接受骨锚定环形闭合装置(ACD)额外植入组(n=272)或不接受额外植入对照组(n=278)。在 3 年的随访中,主要结果是有症状的椎间盘突出复发、再次手术以及达到腿部疼痛、Oswestry 功能障碍指数(ODI)、SF-36 生理成分综合评分(PCS)和 SF-36 心理成分综合评分(MCS)最小临床重要差异(MCID)而无需再次手术的患者比例。比较了老年(≥60 岁)和年轻(<60 岁)患者的结果。我们还分析了两个 ACD 上市后注册研究的数据,以确定随机试验和上市后真实世界结果之间结果的一致性。在所有患者中,老年患者术前残疾更为严重,经常需要卧床或坐轮椅(57.9%比 39.1%,=0.03)。在对照组中,女性、较高的术前 ODI 和当前吸烟状态,但不是年龄,与椎间盘突出复发和再次手术的风险增加相关。与对照组相比,ACD 组有较低的症状性椎间盘突出复发风险(HR=0.45,<0.001)和再次手术风险(HR=0.54,=0.008),且在老年患者和年轻患者中风险降低程度相当。在 ACD 组中,不进行再次手术而达到 MCID 的患者比例在腿部疼痛(81%比 72%,=0.04)、ODI(82%比 73%,=0.03)、PCS(85%比 75%,=0.01)和 MCS(59%比 46%,=0.007)方面更高,且在老年患者和年轻患者中获益程度相当。在 ACD 上市后注册研究中观察到老年患者有类似的获益。与单独腰椎间盘切除术相比,腰椎间盘切除术和附加骨锚定 ACD 的效果更好。老年患者接受附加骨锚定 ACD 植入的获益与年轻患者相似。