van den Brink Wimar, Flüh Charlotte, Miller Larry E, Klassen Peter Douglas, Bostelmann Richard
Neurochirurgisch Centrum Zwolle, Zwolle, The Netherlands.
Department of Neurosurgery, University Medical Center Schleswig-Holstein, Campus Kiel, Kiel, Germany.
Medicine (Baltimore). 2019 Nov;98(44):e17760. doi: 10.1097/MD.0000000000017760.
The risk of recurrent herniation after lumbar discectomy is highest during the first postoperative year. The purpose of this study was to determine whether implantation of a bone-anchored annular closure device (ACD) following limited lumbar discectomy reduced the risk of recurrent herniation and complications during the first year of follow-up compared to limited lumbar discectomy alone (Controls) and whether this risk was influenced by patient characteristics.
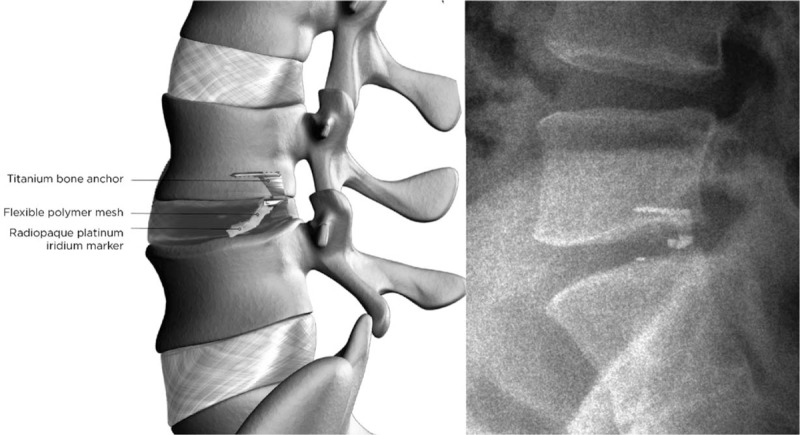
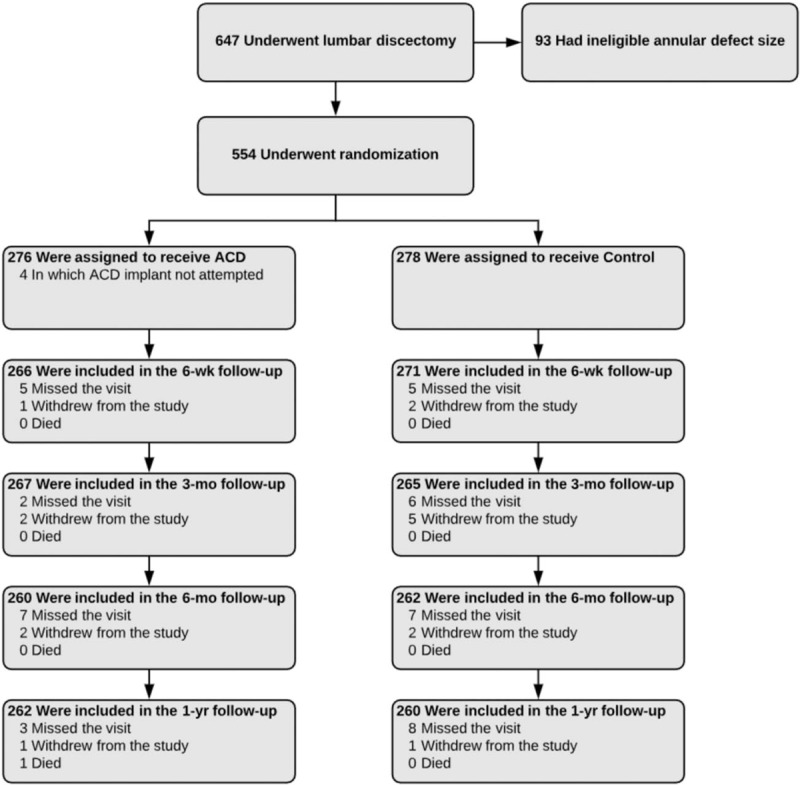
In this randomized multicenter trial, patients with symptomatic lumbar disc herniation and with a large annular defect following limited lumbar discectomy were randomized to bone-anchored ACD or Control groups. The risks of symptomatic reherniation, reoperation, and device- or procedure-related serious adverse events were reported over 1 year of follow-up.
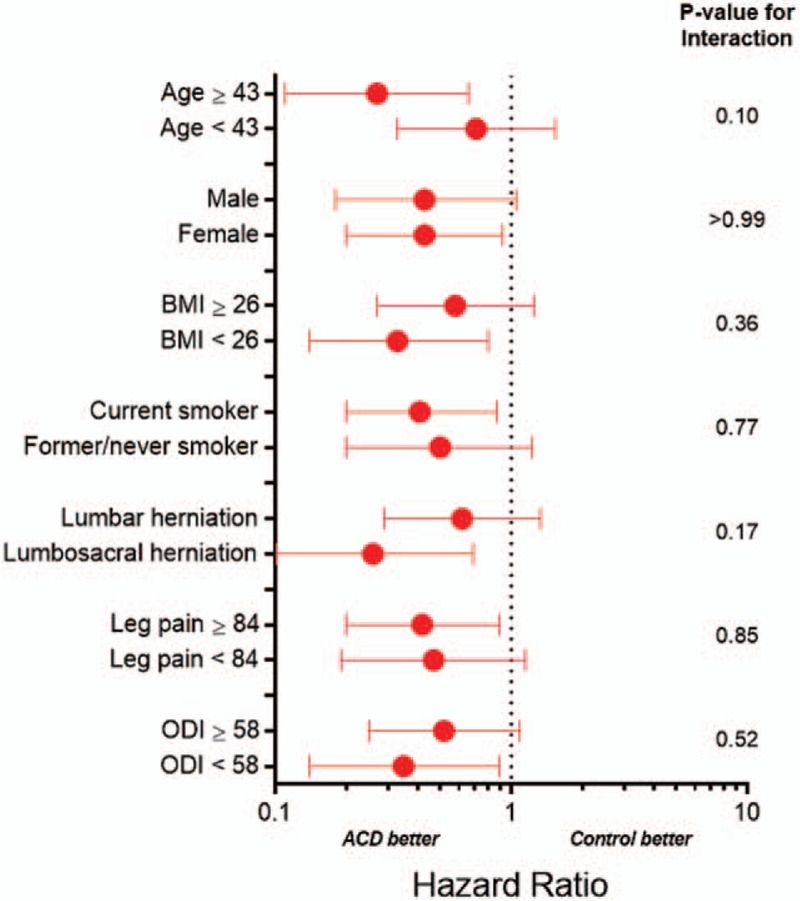
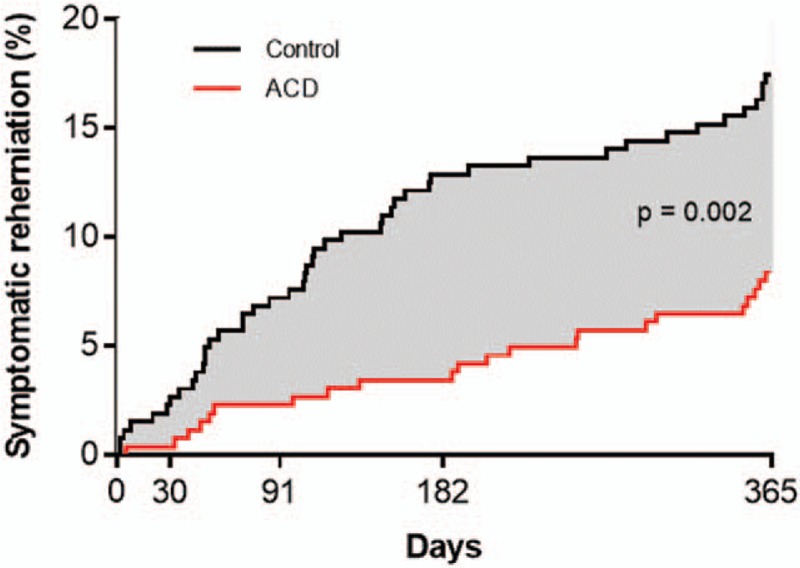
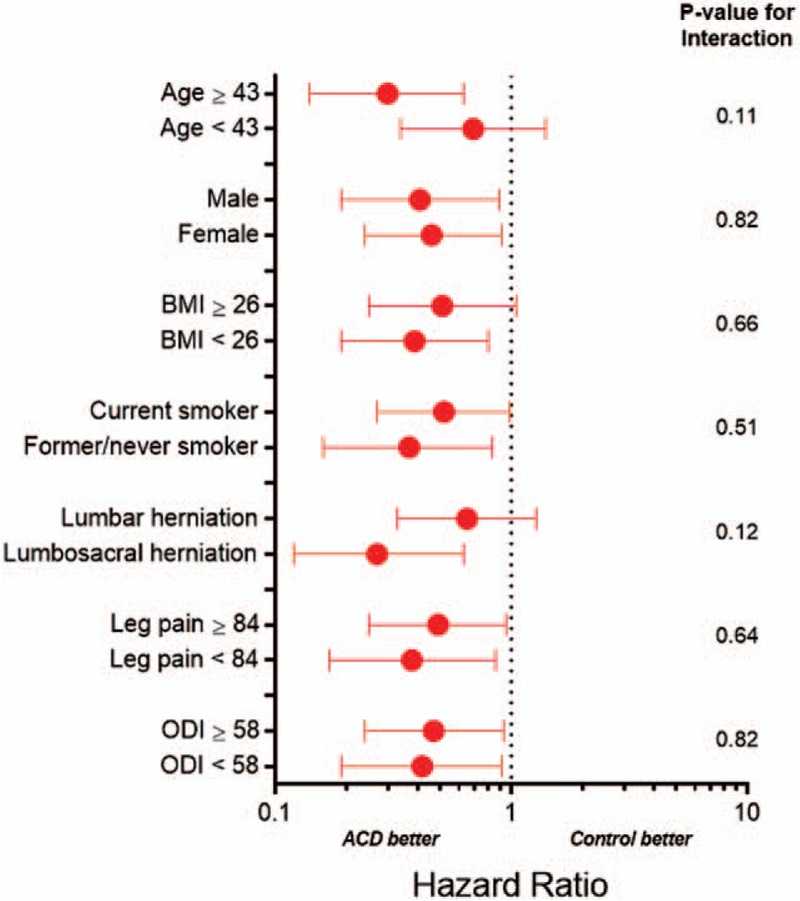
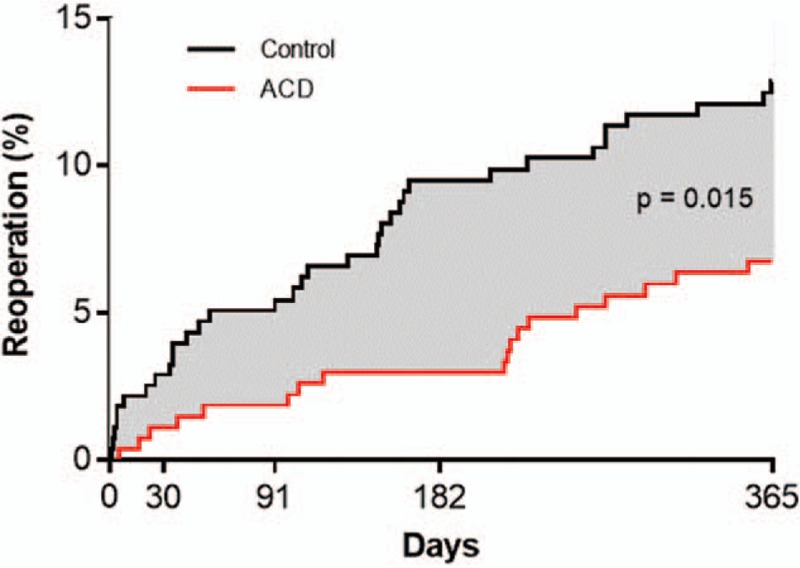
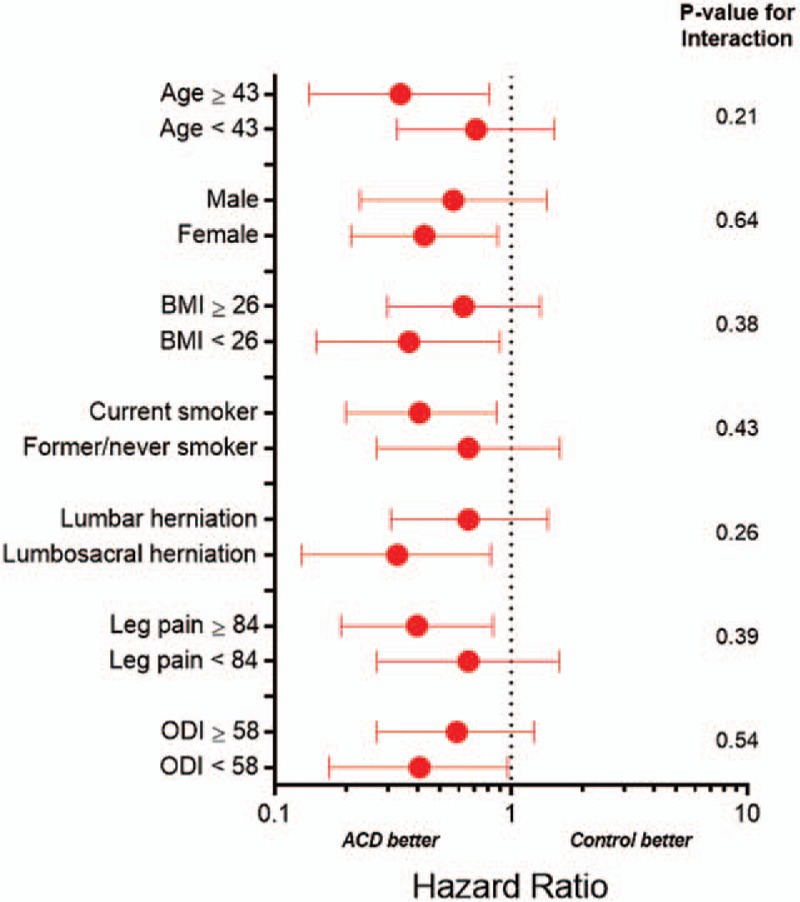
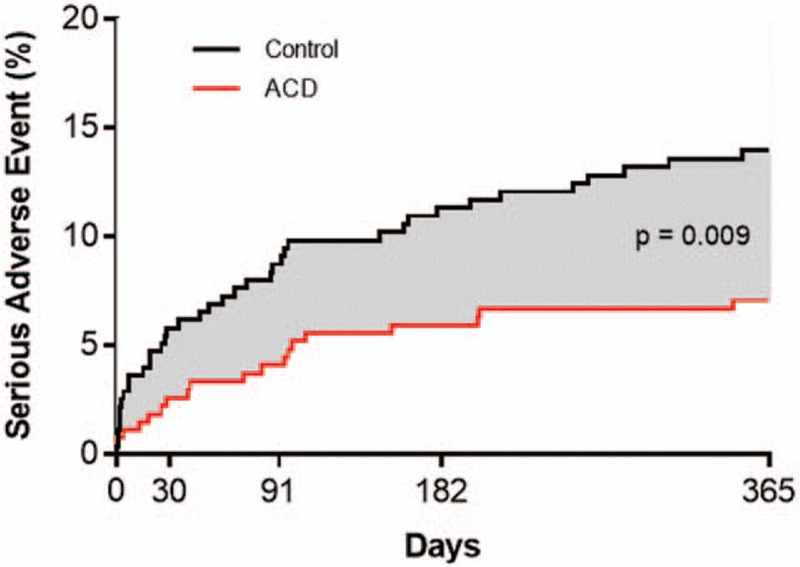
Among 554 patients (ACD 276; Control 278), 94% returned for 1-year follow-up. Bone-anchored ACD resulted in lower risks of symptomatic reherniation (8.4% vs. 17.3%, P = .002) and reoperation (6.7% vs. 12.9%, P = .015) versus Controls. Device- or procedure-related serious adverse events through 1 year were reported in 7.1% of ACD patients and 13.9% of Controls (P = .009). No baseline patient characteristic significantly influenced these risks.
Among patients with large annular defects following limited lumbar discectomy, additional implantation with a bone-anchored ACD lowered the risk of symptomatic reherniation and reoperation over 1 year follow-up. Device- or procedure-related serious adverse events occurred less frequently in the ACD group. These conclusions were not influenced by patient characteristics. ClinicalTrials.gov (NCT01283438).
腰椎间盘切除术后复发疝的风险在术后第一年最高。本研究的目的是确定与单纯有限腰椎间盘切除术(对照组)相比,有限腰椎间盘切除术后植入骨锚定环形闭合装置(ACD)是否能降低随访第一年复发疝和并发症的风险,以及这种风险是否受患者特征的影响。
在这项随机多中心试验中,有症状的腰椎间盘突出症且有限腰椎间盘切除术后存在大的环形缺损的患者被随机分为骨锚定ACD组或对照组。在1年的随访中报告了有症状的再疝、再次手术以及与装置或手术相关的严重不良事件的风险。
554例患者(ACD组276例;对照组278例)中,94%返回进行1年随访。与对照组相比,骨锚定ACD导致有症状的再疝风险(8.4%对17.3%,P = 0.002)和再次手术风险(6.7%对12.9%,P = 0.015)更低。1年内,7.1%的ACD组患者和13.9%的对照组患者报告了与装置或手术相关的严重不良事件(P = 0.009)。没有基线患者特征显著影响这些风险。
在有限腰椎间盘切除术后存在大的环形缺损的患者中,额外植入骨锚定ACD可降低1年随访期间有症状的再疝和再次手术的风险。ACD组与装置或手术相关的严重不良事件发生频率较低。这些结论不受患者特征的影响。ClinicalTrials.gov(NCT01283438)。