Derksen Jeroen W G, Kurk Sophie A, Oskam Marieke J, Peeters Petra H M, Punt Cornelis J A, Koopman Miriam, May Anne M
Department of Medical Oncology, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
Department of Epidemiology, Julius Center for Health Sciences and Primary Care, University Medical Center Utrecht, Utrecht University, Utrecht, the Netherlands.
JNCI Cancer Spectr. 2019 Apr 25;3(2):pkz014. doi: 10.1093/jncics/pkz016. eCollection 2019 Jun.
Increasing evidence indicates that loss of muscle mass is associated with adverse outcomes in metastatic colorectal cancer. Here, we investigate which demographic, lifestyle- (smoking), tumor-, and treatment-related factors are associated with muscle loss in patients with metastatic colorectal cancer during first-line palliative systemic treatment.
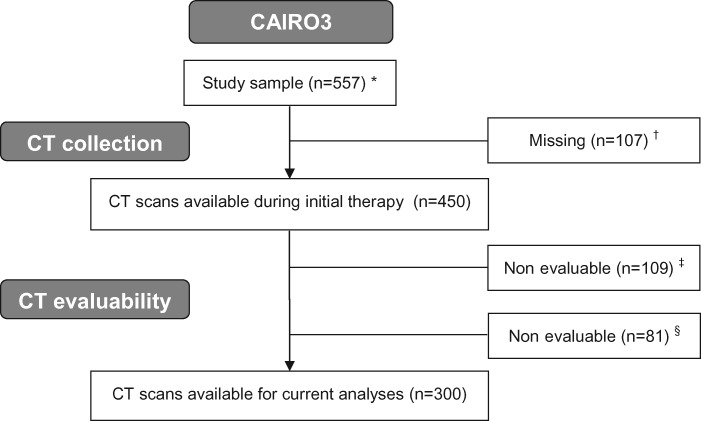
Data from 300 patients with computed tomography scans both at start and after six initial cycles of capecitabine plus oxaliplatin and bevacizumab was used (CAIRO3). From computed tomography, muscle mass normalized for stature (skeletal muscle index [SMI]) was calculated. A priori-selected variables were tested using multivariable linear regression models ( values ≤.05). Two models were developed: Model 1 contained variables measured at start and Model 2 contained variables assessed after initial therapy.
In Model 1, loss of SMI was statistically significantly associated with a higher initial SMI (-0.32%, 95% confidence interval [CI] = -0.45% to -0.19% per unit increase in initial SMI), smoking status (-2.74%, 95% CI = -5.29% to -0.19% for smokers), and interval of metastases (-3.02%, 95% CI = -5.50% to -0.53%) for metachronous vs synchronous metastases), and primary tumor resection was statistically significantly associated with a gain in SMI (2.17%, 95% CI = 0.13% to 4.21% for resection vs no resection). In Model 2, loss of SMI was statistically significantly associated with response to capecitabine plus oxaliplatin and bevacizumab (-2.48%, 95% CI = -4.33% to -0.62% for stable disease vs partial/complete response).
Our results highlight, given the association of sarcopenia and survival, that patients with higher SMI should not be ignored. In addition, smoking is a potentially modifiable factor associated with muscle loss. The association between smoking and muscle loss might relate to worse clinical outcomes in smokers with metastatic colorectal cancer.
越来越多的证据表明,肌肉量减少与转移性结直肠癌的不良预后相关。在此,我们研究在一线姑息性全身治疗期间,哪些人口统计学、生活方式(吸烟)、肿瘤及治疗相关因素与转移性结直肠癌患者的肌肉量减少有关。
使用来自300例患者的数据,这些患者在开始接受卡培他滨加奥沙利铂和贝伐单抗治疗以及初始六个周期治疗后均进行了计算机断层扫描(CAIRO3研究)。根据计算机断层扫描计算出身高标准化的肌肉量(骨骼肌指数[SMI])。使用多变量线性回归模型对预先选定的变量进行检验(P值≤0.05)。构建了两个模型:模型1包含开始时测量的变量,模型2包含初始治疗后评估的变量。
在模型1中,SMI降低与较高的初始SMI(初始SMI每增加一个单位,降低-0.32%,95%置信区间[CI]=-0.45%至-0.19%)、吸烟状况(吸烟者为-2.74%,95%CI=-5.29%至-0.19%)以及异时性转移与同时性转移相比的转移间隔(-3.02%,95%CI=-5.50%至-0.53%)具有统计学显著相关性,并且原发性肿瘤切除与SMI增加具有统计学显著相关性(切除与未切除相比为2.17%,95%CI=0.13%至4.21%)。在模型2中,SMI降低与对卡培他滨加奥沙利铂和贝伐单抗的反应具有统计学显著相关性(疾病稳定与部分/完全缓解相比为-2.48%,95%CI=-4.33%至-0.62%)。
鉴于肌肉减少症与生存的关联,我们的结果强调,不应忽视SMI较高的患者。此外,吸烟是与肌肉量减少相关的一个潜在可改变因素。吸烟与肌肉量减少之间的关联可能与转移性结直肠癌吸烟者更差的临床结局有关。