Mayo Clinic School of Graduate Medical Education.
Biomedical Ethics Program.
Clin J Am Soc Nephrol. 2019 Aug 7;14(8):1213-1227. doi: 10.2215/CJN.00050119. Epub 2019 Jul 30.
Dialysis is a preference-sensitive decision where prognosis may play an important role. Although patients desire risk prediction, nephrologists are wary of sharing this information. We reviewed the performance of prognostic indices for patients starting dialysis to facilitate bedside translation.
DESIGN, SETTING, PARTICIPANTS, & MEASUREMENTS: Systematic review and meta-analysis following the PRISMA guidelines. We searched Ovid MEDLINE, Ovid Embase, Ovid Central Register of Controlled Trials, Ovid Cochrane Database of Systematic Reviews, and Scopus for eligible studies of patients starting dialysis published from inception to December 31, 2018.
Articles describing validated prognostic indices predicting mortality at the start of dialysis. We excluded studies limited to prevalent dialysis patients, AKI and studies excluding mortality in the first 1-3 months. Two reviewers independently screened abstracts, performed full text assessment of inclusion criteria and extracted: study design, setting, population demographics, index performance and risk of bias. Pre-planned random effects meta-analysis was performed stratified by index and predictive window to reduce heterogeneity.
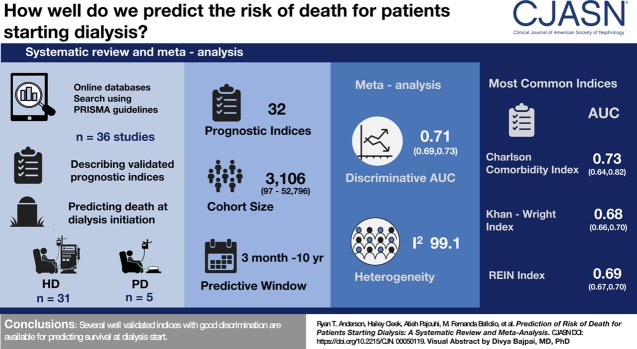
Of 12,132 articles screened and 214 reviewed in full text, 36 studies were included describing 32 prognostic indices. Predictive windows ranged from 3 months to 10 years, cohort sizes from 46 to 52,796. Meta-analysis showed discrimination area under the curve (AUC) of 0.71 (95% confidence interval, 0.69 to 073) with high heterogeneity (=99.12). Meta-analysis by index showed highest AUC for The Obi, Ivory, and Charlson comorbidity index (CCI)=0.74, also CCI was the most commonly used (ten studies). Other commonly used indices were Kahn-Wright index (eight studies, AUC 0.68), Hemmelgarn modification of the CCI (six studies, AUC 0.66) and REIN index (five studies, AUC 0.69). Of the indices, ten have been validated externally, 16 internally and nine were pre-existing validated indices. Limitations include heterogeneity and exclusion of large cohort studies in prevalent patients.
Several well validated indices with good discrimination are available for predicting survival at dialysis start.
透析是一种偏好敏感的决策,预后可能在此过程中扮演着重要的角色。尽管患者希望对预后风险进行预测,但肾脏科医生却对此持谨慎态度,不愿与患者分享这些信息。我们对开始透析的患者的预后指标进行了回顾,以促进其在床旁的转化应用。
设计、地点、参与者和测量方法:遵循 PRISMA 指南进行系统综述和荟萃分析。我们在 Ovid MEDLINE、Ovid Embase、Ovid 中央对照试验注册库、Ovid Cochrane 系统评价数据库和 Scopus 中搜索了从开始到 2018 年 12 月 31 日发表的关于开始透析患者的合格研究,这些研究均描述了用于预测死亡率的验证后的预后指标。
描述用于预测开始透析时死亡率的验证后的预后指标的研究。我们排除了仅限于现患透析患者、急性肾损伤和排除了前 1-3 个月内死亡率的研究。两名审查员独立筛选摘要,并对纳入标准的全文评估进行了评估,并提取了:研究设计、地点、人群统计学、指标表现和偏倚风险。根据指标和预测窗口进行了预先计划的随机效应荟萃分析,以减少异质性。
在筛选出的 12132 篇文章中,有 214 篇文章经过全文评估,其中 36 项研究被纳入,共描述了 32 项预后指标。预测窗口范围从 3 个月到 10 年,队列规模从 46 到 52796 不等。荟萃分析显示,曲线下面积(AUC)的判别率为 0.71(95%置信区间,0.69-0.73),且存在高度异质性(=99.12)。根据指标进行的荟萃分析显示,Obi、Ivory 和 Charlson 合并症指数(CCI)的 AUC 最高(=0.74),CCI 也是最常用的指标(10 项研究)。其他常用的指标包括 Kahn-Wright 指数(8 项研究,AUC=0.68)、Hemmelgarn 对 CCI 的修正(6 项研究,AUC=0.66)和 REIN 指数(5 项研究,AUC=0.69)。在这些指标中,有 10 项指标已经在外部进行了验证,16 项指标在内部进行了验证,9 项指标是预先存在的已验证的指标。其局限性包括异质性和排除了大量现患患者的队列研究。
有一些经过良好验证且具有良好判别能力的指标可用于预测透析开始时的生存情况。