Division of Community Internal Medicine, Department of Medicine, Mayo Clinic, Rochester, Minnesota, United States of America.
Biomedical Ethics Program, Mayo Clinic, Rochester, Minnesota, United States of America.
PLoS One. 2021 Jan 20;16(1):e0244081. doi: 10.1371/journal.pone.0244081. eCollection 2021.
Prognosis provides critical knowledge for shared decision making between patients and clinicians. While several prognostic indices for mortality in dialysis patients have been developed, their performance among elderly patients initiating dialysis is unknown, despite great need for reliable prognostication in that context. To assess the performance of 6 previously validated prognostic indices to predict 3 and/or 6 months mortality in a cohort of elderly incident dialysis patients.
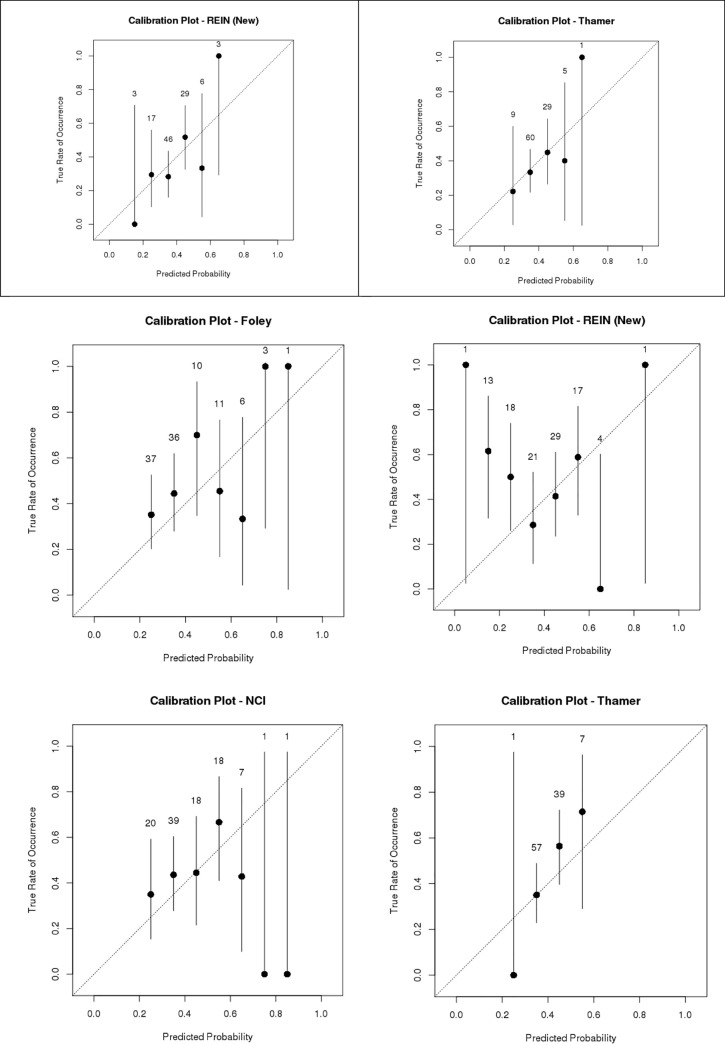
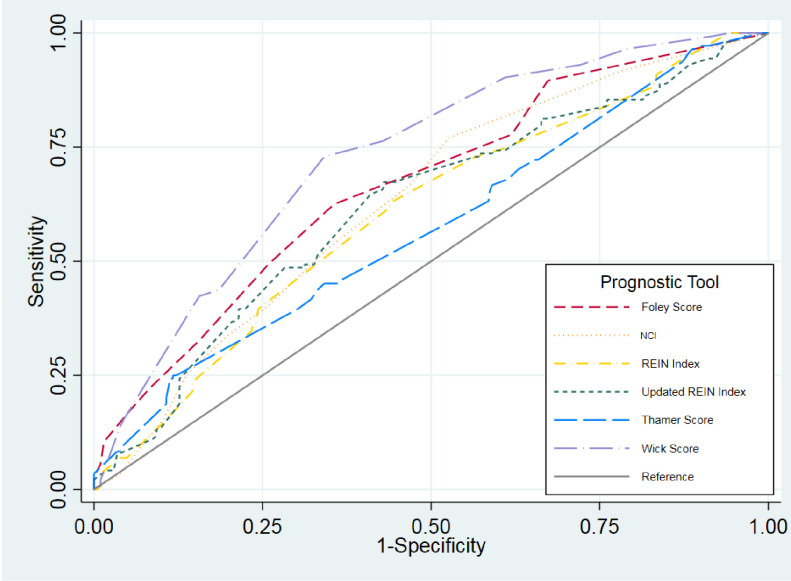
Validation study of prognostic indices using retrospective cohort data. Indices were compared using the concordance ("c")-statistic, i.e. area under the receiver operating characteristic curve (ROC). Calibration, sensitivity, specificity, positive and negative predictive values were also calculated.
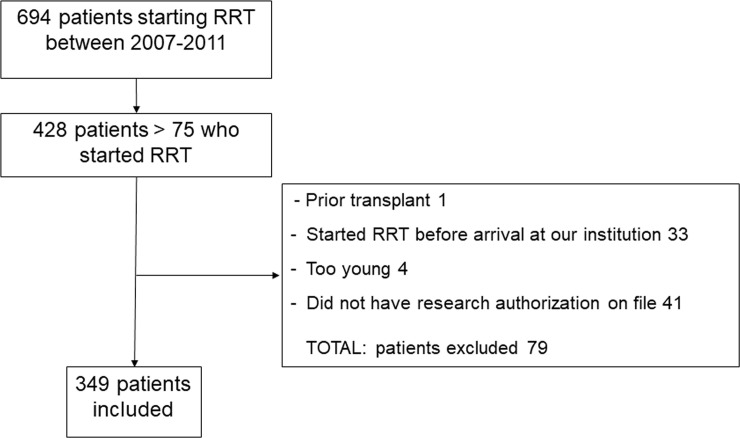
SETTING & PARTICIPANTS: Incident elderly (age ≥75 years; n = 349) dialysis patients at a tertiary referral center.
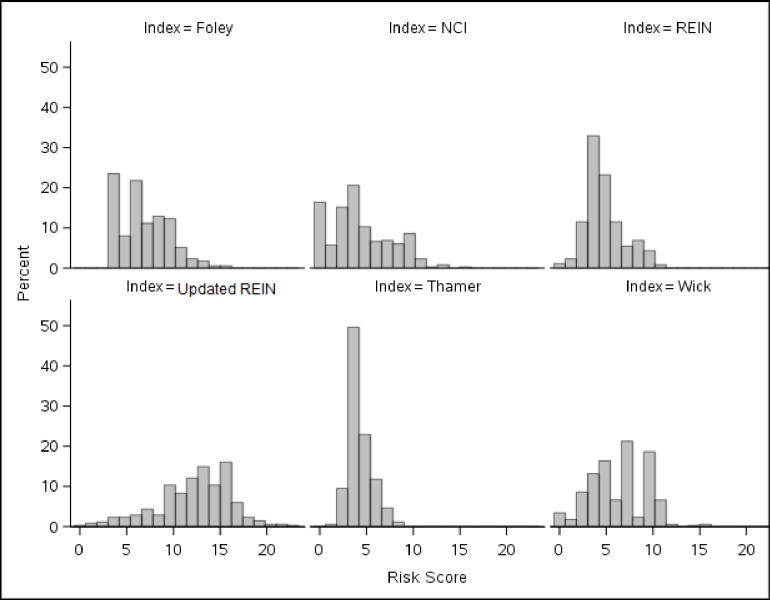
Variables for six validated prognostic indices for short term (3 and 6 month) mortality prediction (Foley, NCI, REIN, updated REIN, Thamer, and Wick) were extracted from the electronic medical record. The indices were individually applied as per each index specifications to predict 3- and/or 6-month mortality.
In our cohort of 349 patients, mean age was 81.5±4.4 years, 66% were male, and median survival was 351 days. The c-statistic for the risk prediction indices ranged from 0.57 to 0.73. Wick ROC 0.73 (0.68, 0.78) and Foley 0.67 (0.61, 0.73) indices performed best. The Foley index was weakly calibrated with poor overall model fit (p <0.01) and overestimated mortality risk, while the Wick index was relatively well-calibrated but underestimated mortality risk.
Small sample size, use of secondary data, need for imputation, homogeneous population.
Most predictive indices for mortality performed moderately in our incident dialysis population. The Wick and Foley indices were the best performing, but had issues with under and over calibration. More accurate indices for predicting survival in older patients with kidney failure are needed.
预后为患者和临床医生之间的共同决策提供了关键信息。虽然已经开发出几种用于预测透析患者死亡率的预后指数,但在开始透析的老年患者中,这些指数的表现尚不清楚,尽管在这种情况下非常需要可靠的预后判断。评估 6 种先前验证的预后指数在老年新透析患者队列中预测 3 个月和/或 6 个月死亡率的表现。
使用回顾性队列数据验证预后指数的研究。使用一致性(“c”)-统计量,即接受者操作特征曲线(ROC)下的面积来比较指数。还计算了校准、敏感性、特异性、阳性和阴性预测值。
三级转诊中心的新发生的老年(年龄≥75 岁;n=349)透析患者。
从电子病历中提取了用于短期(3 个月和 6 个月)死亡率预测的 6 种经过验证的预后指数(Foley、NCI、REIN、更新的 REIN、Thamer 和 Wick)的变量。根据每个指数的规格将指数单独应用于预测 3 个月和/或 6 个月的死亡率。
在我们的 349 名患者队列中,平均年龄为 81.5±4.4 岁,66%为男性,中位生存时间为 351 天。风险预测指数的 c 统计量范围为 0.57 至 0.73。Wick ROC 0.73(0.68,0.78)和 Foley 0.67(0.61,0.73)指数表现最佳。Foley 指数校准效果较弱,整体模型拟合不佳(p<0.01)且高估了死亡率风险,而 Wick 指数则相对较好校准但低估了死亡率风险。
样本量小、使用二次数据、需要插补、人群同质。
在我们的新透析人群中,大多数用于预测死亡率的预测指标表现中等。Wick 和 Foley 指数表现最好,但存在校准不足和过度校准的问题。需要更准确的指数来预测肾衰竭老年患者的生存。