From the Department of Pediatrics (K.M., T.N.W.) and Nutrition Research Section (G.F.), Imperial College London, and the Medical Research Council Clinical Trials Unit at University College London (E.C.G., D.M.G., A.S.W.), London, the Centre for Health Economics, University of York, York (P.S.G.), the School of Medicine, Dentistry, and Biomedical Science, Queen's University, Belfast (N.K.), Liverpool School of Tropical Medicine and Hygiene, Liverpool (I.B.), and the Department of Pediatrics, University Hospital of Wales, Cardiff (J.A.E.) - all in the United Kingdom; the Department of Pediatrics, Makerere University and Mulago Hospital (S.K., R.O.O., E.N.), and the Uganda Blood Transfusion Services (BTS), National BTS (D.K.B.), Kampala, Busitema University Faculty of Health Sciences, Mbale Campus and Mbale Regional Referral Hospital (P.O.-O., J.N., C.N.), and Mbale BTS (B.W.), Mbale, and the Soroti Regional Referral Hospital, Soroti (C.E., F.A., M.N.) - all in Uganda; the College of Medicine and Malawi-Liverpool-Wellcome Trust Clinical Research Program (M.M., G.C.). and Malawi BTS (B.M.), Blantyre, Malawi; and the Kenya Medical Research Institute-Wellcome Trust Research Program, Kilifi, Kenya (K.M., A.M. S.U., T.N.W.).
N Engl J Med. 2019 Aug 1;381(5):407-419. doi: 10.1056/NEJMoa1900105.
The World Health Organization recommends not performing transfusions in African children hospitalized for uncomplicated severe anemia (hemoglobin level of 4 to 6 g per deciliter and no signs of clinical severity). However, high mortality and readmission rates suggest that less restrictive transfusion strategies might improve outcomes.
In this factorial, open-label, randomized, controlled trial, we assigned Ugandan and Malawian children 2 months to 12 years of age with uncomplicated severe anemia to immediate transfusion with 20 ml or 30 ml of whole-blood equivalent per kilogram of body weight, as determined in a second simultaneous randomization, or no immediate transfusion (control group), in which transfusion with 20 ml of whole-blood equivalent per kilogram was triggered by new signs of clinical severity or a drop in hemoglobin to below 4 g per deciliter. The primary outcome was 28-day mortality. Three other randomizations investigated transfusion volume, postdischarge supplementation with micronutrients, and postdischarge prophylaxis with trimethoprim-sulfamethoxazole.
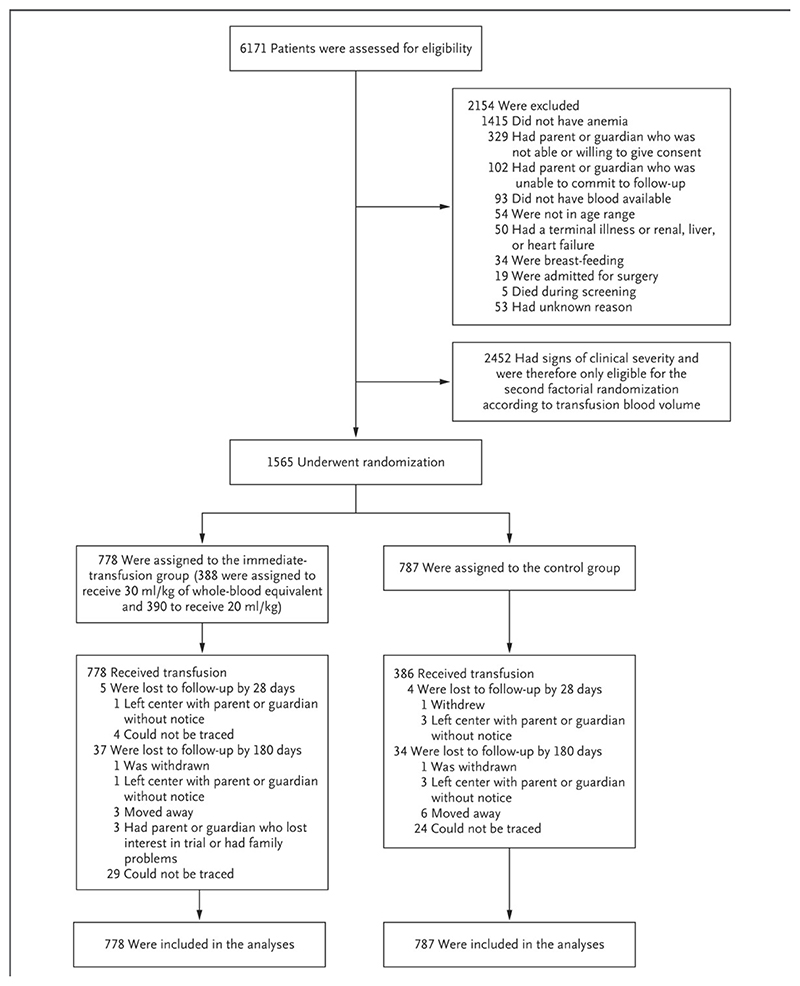
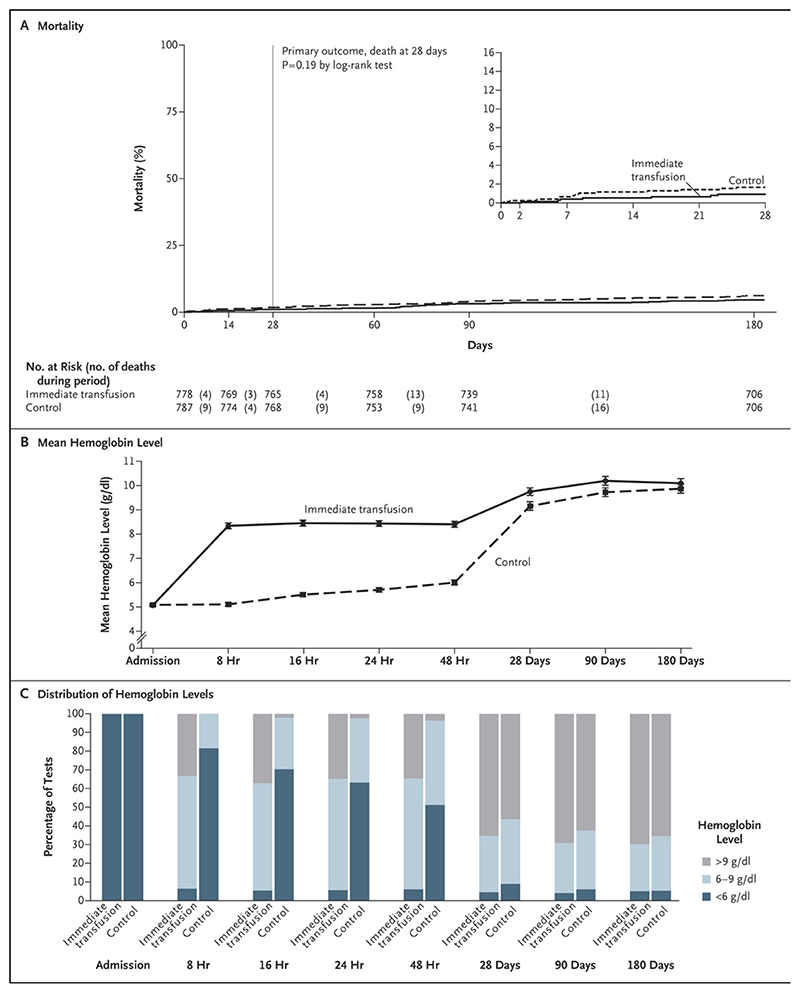
A total of 1565 children (median age, 26 months) underwent randomization, with 778 assigned to the immediate-transfusion group and 787 to the control group; 984 children (62.9%) had malaria. The children were followed for 180 days, and 71 (4.5%) were lost to follow-up. During the primary hospitalization, transfusion was performed in all the children in the immediate-transfusion group and in 386 (49.0%) in the control group (median time to transfusion, 1.3 hours vs. 24.9 hours after randomization). The mean (±SD) total blood volume transfused per child was 314±228 ml in the immediate-transfusion group and 142±224 ml in the control group. Death had occurred by 28 days in 7 children (0.9%) in the immediate-transfusion group and in 13 (1.7%) in the control group (hazard ratio, 0.54; 95% confidence interval [CI], 0.22 to 1.36; P = 0.19) and by 180 days in 35 (4.5%) and 47 (6.0%), respectively (hazard ratio, 0.75; 95% CI, 0.48 to 1.15), without evidence of interaction with other randomizations (P>0.20) or evidence of between-group differences in readmissions, serious adverse events, or hemoglobin recovery at 180 days. The mean length of hospital stay was 0.9 days longer in the control group.
There was no evidence of differences in clinical outcomes over 6 months between the children who received immediate transfusion and those who did not. The triggered-transfusion strategy in the control group resulted in lower blood use; however, the length of hospital stay was longer, and this strategy required clinical and hemoglobin monitoring. (Funded by the Medical Research Council and Department for International Development; TRACT Current Controlled Trials number, ISRCTN84086586.).
世界卫生组织建议,在非洲患有非复杂性严重贫血(血红蛋白水平为每分升 4 至 6 克且无临床严重程度迹象)的住院儿童中不进行输血。然而,高死亡率和再入院率表明,限制较少的输血策略可能会改善预后。
在这项两因素、开放标签、随机对照试验中,我们将乌干达和马拉维 2 个月至 12 岁患有非复杂性严重贫血的儿童随机分为立即输血组(立即输血组)和对照组(无立即输血组)。立即输血组根据第二次同时随机化,用相当于每公斤 20 或 30 毫升全血的量输血;对照组用相当于每公斤 20 毫升全血的量输血,当出现新的临床严重程度迹象或血红蛋白下降至每分升 4 克以下时触发输血。主要结局为 28 天死亡率。另外三次随机化分别研究了输血量、出院后补充微量营养素和出院后用甲氧苄啶-磺胺甲噁唑进行预防。
共有 1565 名儿童(中位数年龄为 26 个月)接受了随机分组,其中 778 名被分配到立即输血组,787 名被分配到对照组;984 名儿童(62.9%)患有疟疾。对这些儿童进行了 180 天的随访,其中有 71 名(4.5%)失访。在初次住院期间,立即输血组所有儿童均进行了输血,对照组中 386 名(49.0%)进行了输血(中位输血时间为随机分组后 1.3 小时与 24.9 小时)。立即输血组中每名儿童的平均(±SD)总输血量为 314±228 毫升,对照组为 142±224 毫升。在立即输血组中,有 7 名(0.9%)儿童在 28 天内死亡,对照组中 13 名(1.7%)儿童死亡(风险比,0.54;95%置信区间 [CI],0.22 至 1.36;P=0.19),180 天时,35 名(4.5%)和 47 名(6.0%)儿童死亡(风险比,0.75;95% CI,0.48 至 1.15),无其他随机分组(P>0.20)或组间差异的证据表明再入院、严重不良事件或 180 天时的血红蛋白恢复情况。对照组的平均住院时间延长了 0.9 天。
在 6 个月的时间里,接受立即输血的儿童和未接受输血的儿童在临床结局方面没有证据表明存在差异。对照组采用的触发式输血策略导致输血量减少;然而,住院时间延长,且这种策略需要进行临床和血红蛋白监测。(由医学研究委员会和国际发展部资助;TRACE 当前对照试验编号,ISRCTN84086586。)