Chinoy A, Wright N, Bone M, Padidela R
Department of Paediatric Endocrinology, Royal Manchester Children’s Hospital, Manchester, UK
Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK
Endocrinol Diabetes Metab Case Rep. 2019 May 30;2019(1):19-0034. doi: 10.1530/EDM-19-0034.
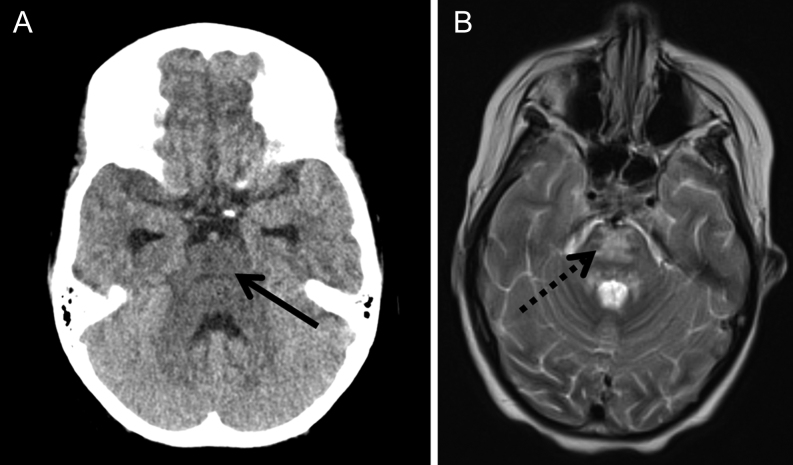
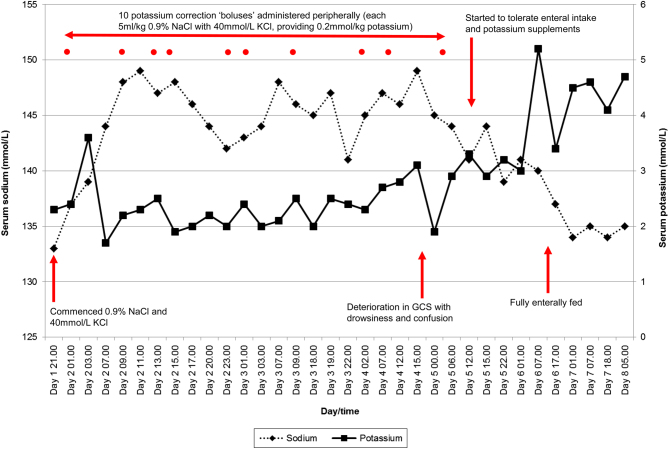
Hypokalaemia at presentation of diabetic ketoacidosis is uncommon as insulin deficiency and metabolic acidosis shifts potassium extracellularly. However, hypokalaemia is a recognised complication of the management of diabetic ketoacidosis as insulin administration and correction of metabolic acidosis shifts potassium intracellularly. We describe the case of a 9-year-old girl with newly diagnosed type 1 diabetes mellitus presenting in diabetic ketoacidosis, with severe hypokalaemia at presentation due to severe and prolonged emesis. After commencing management for her diabetic ketoacidosis, her serum sodium and osmolality increased rapidly. However, despite maximal potassium concentrations running through peripheral access, and multiple intravenous potassium ‘corrections’, her hypokalaemia persisted. Seventy two hours after presentation, she became drowsy and confused, with imaging demonstrating central pontine myelinolysis – a rare entity seldom seen in diabetic ketoacidosis management in children despite rapid shifts in serum sodium and osmolality. We review the literature associating central pontine myelinolysis with hypokalaemia and hypothesise as to how the hypokalaemia may have contributed to the development of central pontine myelinolysis. We also recommend an approach to the management of a child in diabetic ketoacidosis with hypokalaemia at presentation.
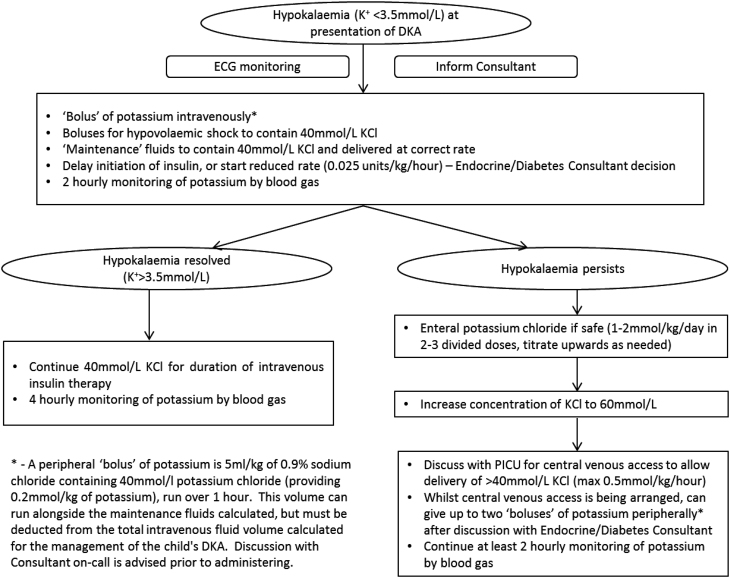
Hypokalaemia is a recognised complication of treatment of paediatric diabetic ketoacidosis that should be aggressively managed to prevent acute complications. Central pontine myelinolysis is rare in children, and usually observed in the presence of rapid correction of hyponatraemia. However, there is observational evidence of an association between hypokalaemia and central pontine myelinolysis, potentially by priming the endothelial cell membrane to injury by lesser fluctuations in osmotic pressure. Consider central pontine myelinolysis as a complication of the management of paediatric diabetic ketoacidosis in the presence of relevant symptoms with profound hypokalaemia and/or fluctuations in serum sodium levels. We have suggested an approach to the management strategies of hypokalaemia in paediatric diabetic ketoacidosis which includes oral potassium supplements if tolerated, minimising the duration and the rate of insulin infusion and increasing the concentration of potassium intravenously (via central line if necessary).
糖尿病酮症酸中毒(DKA)患者出现低钾血症并不常见,因为胰岛素缺乏和代谢性酸中毒会使钾离子向细胞外转移。然而,低钾血症是DKA治疗过程中公认的并发症,因为胰岛素的使用和代谢性酸中毒的纠正会使钾离子向细胞内转移。我们描述了一名9岁新诊断为1型糖尿病的女孩,以DKA就诊,因严重且持续的呕吐在就诊时出现严重低钾血症。在开始对其DKA进行治疗后,她的血清钠和渗透压迅速升高。然而,尽管通过外周静脉通路输入了最大浓度的钾,并多次进行静脉补钾“纠正”,她的低钾血症仍持续存在。就诊72小时后,她变得嗜睡且意识模糊,影像学检查显示为脑桥中央髓鞘溶解症——这是一种在儿童DKA治疗中罕见的病症,尽管血清钠和渗透压快速变化,但仍很少见。我们回顾了将脑桥中央髓鞘溶解症与低钾血症相关联的文献,并推测低钾血症可能如何导致脑桥中央髓鞘溶解症的发生。我们还推荐了一种针对就诊时伴有低钾血症的儿童DKA的管理方法。
低钾血症是小儿糖尿病酮症酸中毒治疗中公认的并发症,应积极处理以预防急性并发症。脑桥中央髓鞘溶解症在儿童中罕见,通常在低钠血症快速纠正的情况下观察到。然而,有观察证据表明低钾血症与脑桥中央髓鞘溶解症之间存在关联,可能是通过使内皮细胞膜更容易受到较小渗透压波动的损伤。在存在严重低钾血症和/或血清钠水平波动的相关症状时,应考虑脑桥中央髓鞘溶解症是小儿糖尿病酮症酸中毒治疗的并发症。我们提出了一种小儿糖尿病酮症酸中毒低钾血症管理策略的方法,包括在耐受的情况下口服补钾,尽量缩短胰岛素输注的持续时间和速率,并增加静脉补钾的浓度(必要时通过中心静脉导管)。