Critical Care Medicine Department, Clinical Center, National Institutes of Health, Bethesda, MD.
NIH Library, National Institutes of Health, Bethesda, MD.
Crit Care Med. 2019 Oct;47(10):1290-1300. doi: 10.1097/CCM.0000000000003892.
To address three controversial components in the Centers for Medicare and Medicaid Service's sepsis bundle for performance measure (SEP-1): antibiotics within 3 hours, a 30 mL/kg fluid infusion for all hypotensive patients, and repeat lactate measurements within 6 hours if initially elevated. We hypothesized that antibiotic- and fluid-focused bundles like SEP-1 would probably show benefit, but evidence supporting specific antibiotic timing, fluid dosing, or serial lactate requirements would not be concordant. Therefore, we performed a meta-analysis of studies of sepsis bundles like SEP-1.
PubMed, Embase, ClinicalTrials.gov through March 15, 2018.
Studies comparing survival in septic adults receiving versus not receiving antibiotic- and fluid-focused bundles.
Two investigators (D.J.P., P.Q.E.).
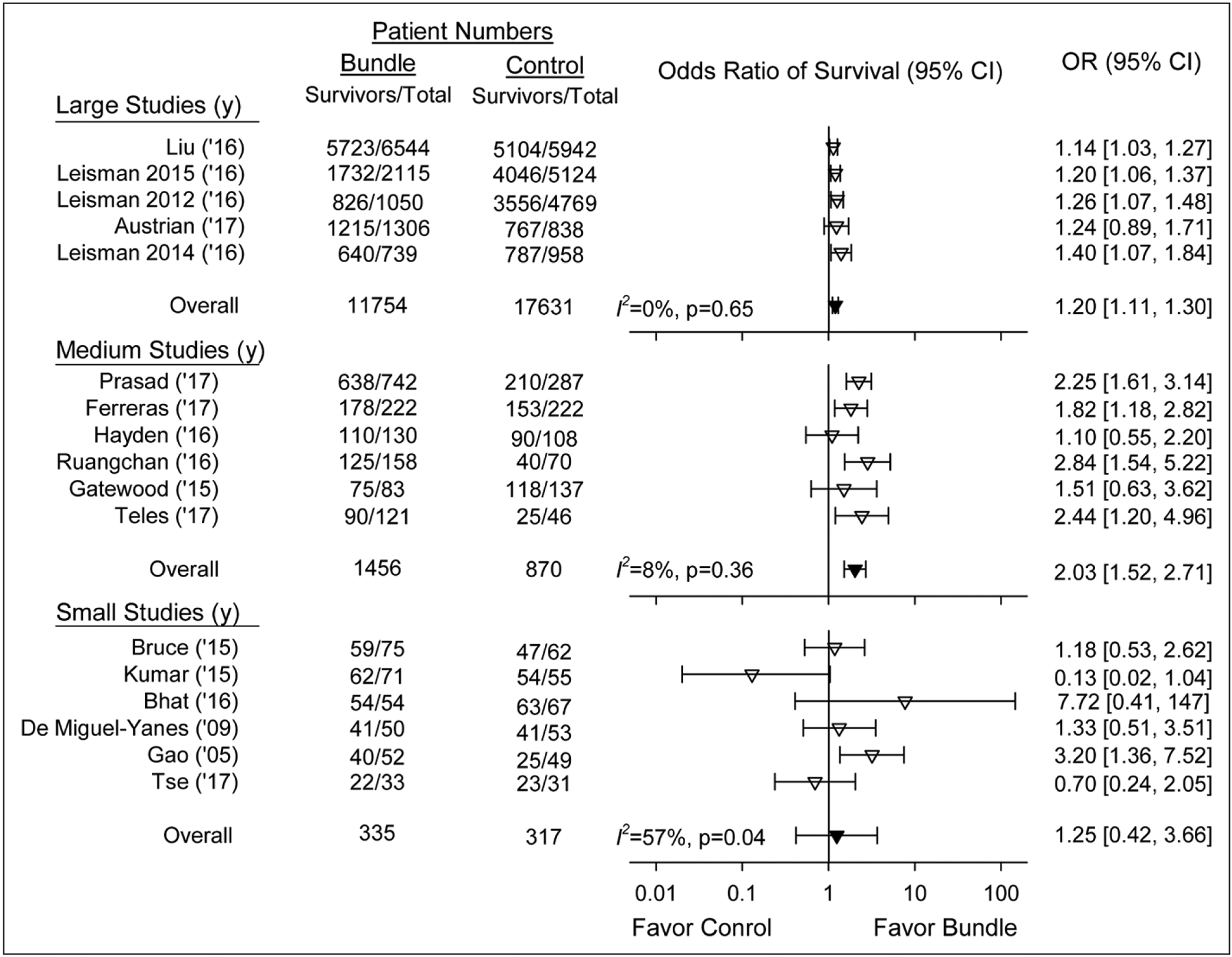
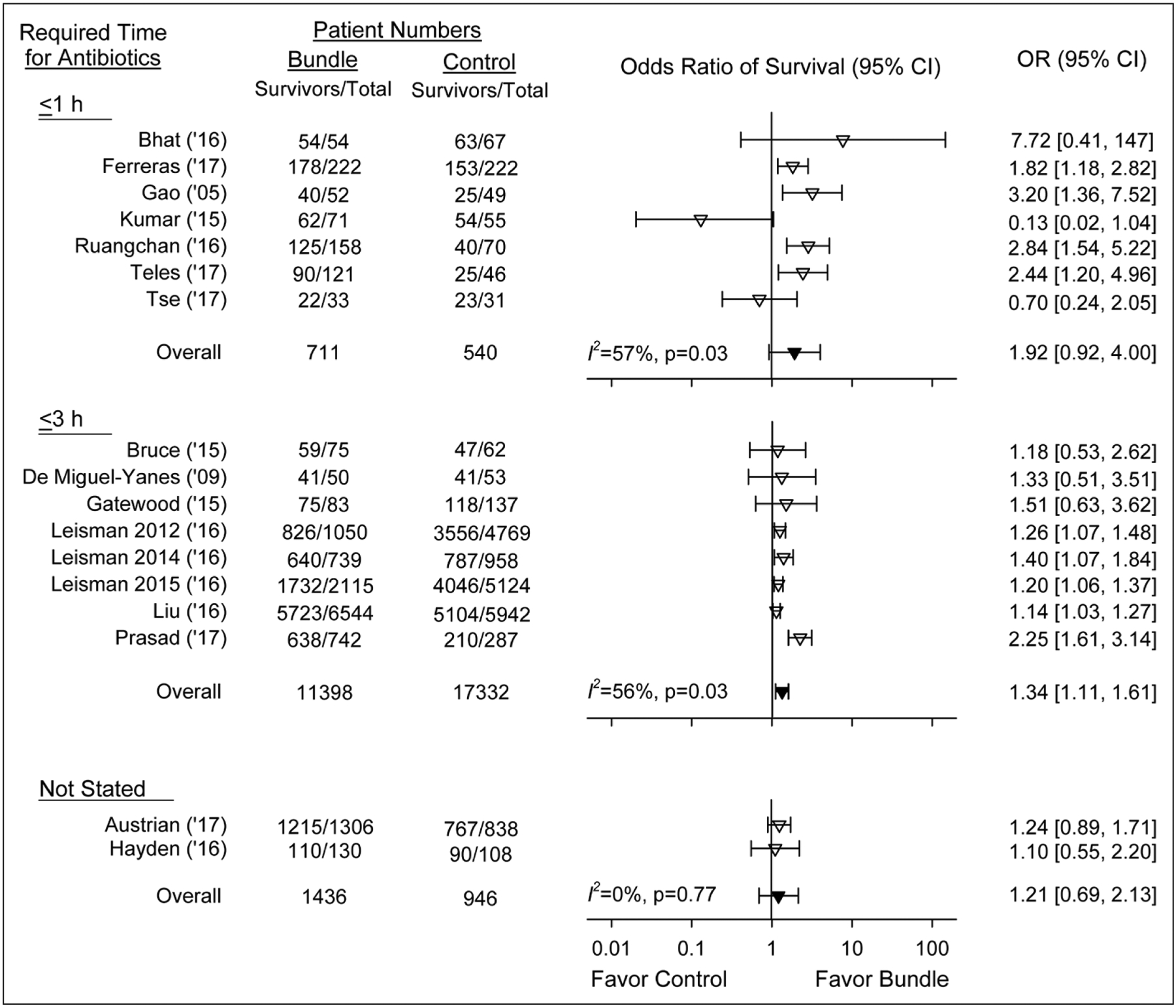
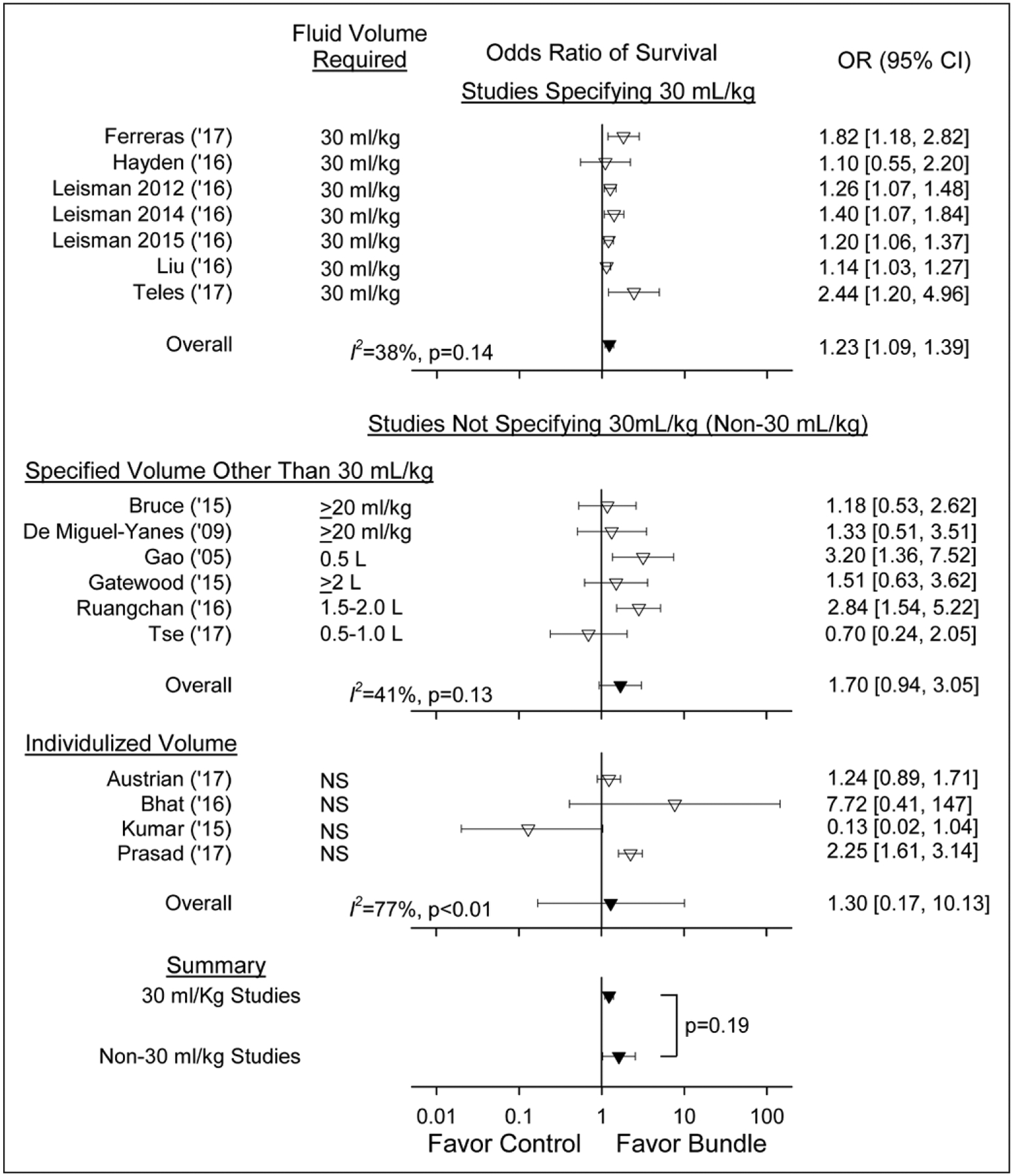
Seventeen observational studies (11,303 controls and 4,977 bundle subjects) met inclusion criteria. Bundles were associated with increased odds ratios of survival (odds ratio [95% CI]) in 15 studies with substantial heterogeneity (I = 61%; p < 0.01). Survival benefits were consistent in the five largest (1,697-12,486 patients per study) (1.20 [1.11-1.30]; I = 0%) and six medium-sized studies (167-1,029) (2.03 [1.52-2.71]; I = 8%) but not the six smallest (64-137) (1.25 [0.42-3.66]; I = 57%). Bundles were associated with similarly increased survival benefits whether requiring antibiotics within 1 hour (n = 7 studies) versus 3 hours (n = 8) versus no specified time (n = 2); or 30 mL/kg fluid (n = 7) versus another volume (≥ 2 L, n = 1; ≥ 20 mL/kg, n = 2; 1.5-2 L or 500 mL, n = 1 each; none specified, n = 4) (p = 0.19 for each comparison). In the only study employing serial lactate measurements, survival was not increased versus others. No study had a low risk of bias or assessed potential adverse bundle effects.
Available studies support the notion that antibiotic- and fluid-focused sepsis bundles like SEP-1 improve survival but do not demonstrate the superiority of any specific antibiotic time or fluid volume or of serial lactate measurements. Until strong reproducible evidence demonstrates the safety and benefit of any fixed requirement for these interventions, the present findings support the revision of SEP-1 to allow flexibility in treatment according to physician judgment.
解决医疗保险和医疗补助服务中心(Centers for Medicare and Medicaid Service)脓毒症捆绑包(SEP-1)中三个有争议的部分:在 3 小时内使用抗生素、所有低血压患者给予 30ml/kg 的液体输注、如果初始乳酸水平升高,则在 6 小时内重复测量乳酸。我们假设像 SEP-1 这样的抗生素和液体为重点的捆绑包可能会显示出获益,但支持特定抗生素使用时机、液体剂量或连续乳酸要求的证据并不一致。因此,我们对类似 SEP-1 的脓毒症捆绑包进行了荟萃分析。
PubMed、Embase、ClinicalTrials.gov,截至 2018 年 3 月 15 日。
比较接受抗生素和液体为重点的捆绑包治疗的脓毒症成人与未接受治疗的存活情况的研究。
两位研究人员(D.J.P.、P.Q.E.)。
符合纳入标准的有 17 项观察性研究(对照组 11303 例,捆绑组 4977 例)。捆绑包与存活的优势比增加相关(15 项研究中,有显著异质性,I=61%,p<0.01)。在五项最大规模的研究(每项研究 1697-12486 例患者)中(1.20[1.11-1.30];I=0%),以及在六项中等规模的研究(167-1029 例患者)中(2.03[1.52-2.71];I=8%),生存获益是一致的,但在六项最小规模的研究(64-137 例患者)中(1.25[0.42-3.66];I=57%)则不然。捆绑包与类似的生存获益相关,无论是否要求在 1 小时(n=7 项研究)内还是 3 小时(n=8 项研究)内使用抗生素,或无具体时间(n=2 项研究);或使用 30ml/kg 液体(n=7 项研究),还是其他容量(≥2L,n=1;≥20ml/kg,n=2;1.5-2L 或 500ml,n=1 项;均未指定,n=4 项)(每项比较的 p=0.19)。在唯一一项采用连续乳酸测量的研究中,与其他研究相比,乳酸水平并未升高。没有研究的偏倚风险低,也没有评估潜在的不良捆绑效应。
现有研究支持这样一种观点,即像 SEP-1 这样的以抗生素和液体为重点的脓毒症捆绑包可以提高存活率,但不能证明任何特定的抗生素使用时间或液体量或连续乳酸测量的优越性。在有强有力的、可重复的证据表明这些干预措施的安全性和获益之前,目前的研究结果支持修订 SEP-1,以根据医生的判断灵活治疗。