Shime Nobuaki, Saito Nobuyuki, Bokui Miya, Sakane Naoki, Kamimura Mitsuhiro, Shinohara Tsutomu, Kosaka Tadashi, Ishikura Hisashi, Kobayashi Atsuko
Department of Emergency and Critical Care Medicine, Graduate School of Biomedical & Health Sciences, Hiroshima University, Hiroshima, Japan,
Department of Emergency and Critical Care Medicine, Kyoto Medical Centre, Kyoto, Japan,
Infect Drug Resist. 2018 Aug 6;11:1073-1081. doi: 10.2147/IDR.S159447. eCollection 2018.
To evaluate the clinical outcomes associated with anti-methicillin-resistant (MRSA) antimicrobials.
We reviewed a prospective database of 247 consecutive patients with clinically and microbiologically confirmed MRSA infections, hospitalized in 7 Japanese hospitals between April 2014 and March 2015, and treated with anti-MRSA pharmaceuticals. Survival was measured at 30 days. We examined the relationships between initial antimicrobial administered and survival and organ toxicity. HR and 95% CIs were calculated.
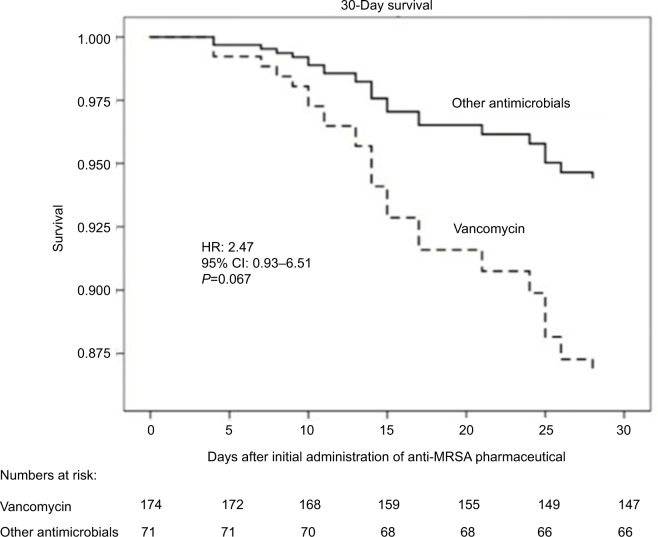
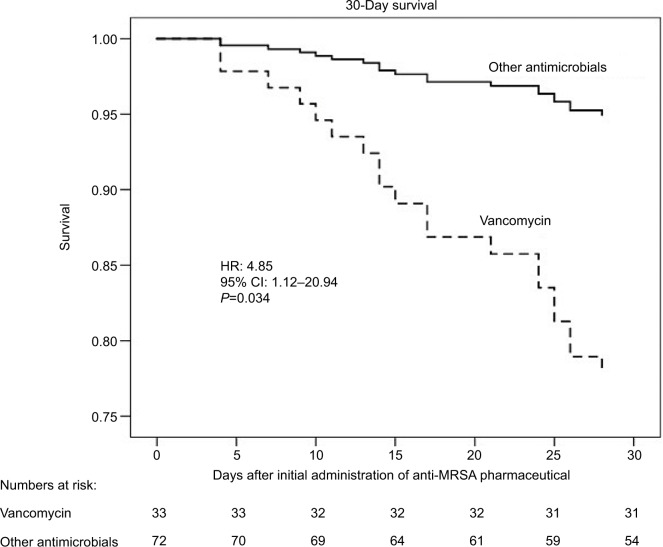
Overall 30-day mortality was 12%. The lungs were infected in 105 (41%), skin and soft tissue in 73 (30%), and bones and joints in 21 (9%) patients. Bacteremia complicated the illness in 69 patients (28%). Among 5 pharmaceuticals, vancomycin was prescribed to 174 (71%), linezolid to 38 (16%), teicoplanin to 22 (9%), and daptomycin to 11 (5%) patients. Vancomycin tended to be associated with the lowest survival (HR=2.47; 95% CI=0.93-6.51; =0.067), particularly in the lung-infected subgroup (HR=4.85; 95% CI=1.12-20.94; =0.034) after adjustments for baseline illness severity. The incidence of renal dysfunction tended to be higher in patients with trough serum concentrations of vancomycin >15 mg/dL.
In this observational study reflecting real-world conditions, vancomycin was associated with higher 30-day mortality and incidence of kidney dysfunction than other anti-MRSA agents. The significance of the differences observed among antimicrobials other than vancomycin is uncertain.
评估与抗耐甲氧西林金黄色葡萄球菌(MRSA)抗菌药物相关的临床结局。
我们回顾了一个前瞻性数据库,该数据库包含2014年4月至2015年3月期间在7家日本医院住院的247例临床和微生物学确诊的MRSA感染患者,并接受了抗MRSA药物治疗。在30天时测量生存率。我们研究了初始使用的抗菌药物与生存率和器官毒性之间的关系。计算了风险比(HR)和95%可信区间(CI)。
总体30天死亡率为12%。105例(41%)患者肺部感染,73例(30%)皮肤和软组织感染,21例(9%)骨骼和关节感染。69例患者(28%)发生菌血症。在5种药物中,174例(71%)患者使用了万古霉素,38例(16%)使用了利奈唑胺,22例(9%)使用了替考拉宁,11例(5%)使用了达托霉素。万古霉素往往与最低的生存率相关(HR=2.47;95%CI=0.93-6.51;P=0.067),特别是在调整基线疾病严重程度后,肺部感染亚组中(HR=4.85;95%CI=1.12-20.94;P=0.034)。万古霉素谷浓度>15mg/dL的患者肾功能不全的发生率往往更高。
在这项反映现实世界情况的观察性研究中,万古霉素与其他抗MRSA药物相比,30天死亡率和肾功能不全发生率更高。除万古霉素外,其他抗菌药物之间观察到的差异的意义尚不确定。