Division of Health Care Policy Research, Mayo Clinic, Rochester, Minnesota.
Department of Anesthesiology and Perioperative Medicine, Mayo Clinic, Rochester, Minnesota.
JAMA Netw Open. 2019 Aug 2;2(8):e198325. doi: 10.1001/jamanetworkopen.2019.8325.
The Centers for Disease Control and Prevention guidelines in 2016 recommended avoiding concurrent use of opioids and benzodiazepines.
To determine whether the release of the guidelines was associated with changes in coprescription of opioids and benzodiazepines.
DESIGN, SETTING, AND PARTICIPANTS: This retrospective cohort study used claims data obtained from a US national database of medical and pharmacy claims for 3 598 322 adult commercially insured patients and 1 299 142 Medicare Advantage (MA) beneficiaries with no recent history of cancer, sickle cell disease, or hospice care who ever used prescribed opioids during the study period, January 1, 2014, through March 31, 2018.
Overlapping opioid and benzodiazepine prescriptions filled.
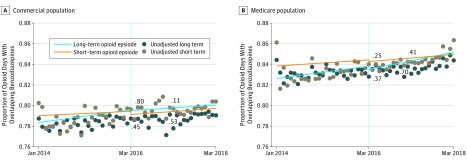
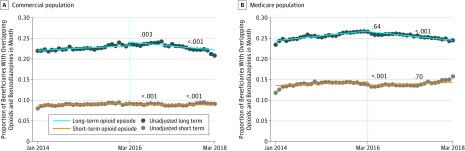
The extent (proportion of person-months with any overlapping days of prescription of opioids and benzodiazepines) and intensity (proportion of days with opioids prescribed where benzodiazepines were also available) of coprescription.
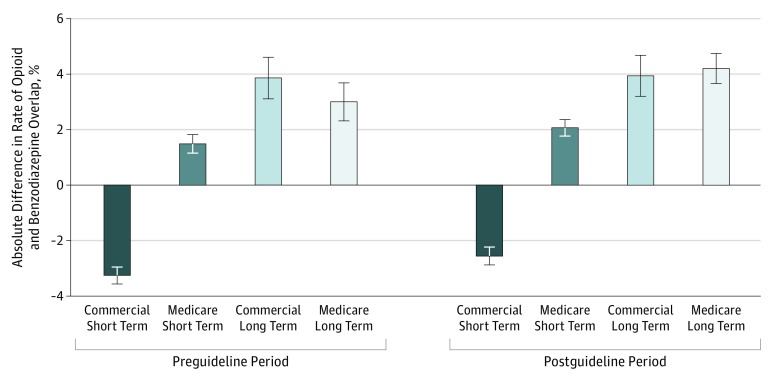
Of 4 897 464 patients (with 13.4 million person-months of opioid use), the total number of unique commercially insured individuals was 3 598 322 (1 974 731 women [54.9%]), and the total number of unique MA beneficiaries was 1 299 142 (770 256 women [59.3%]). Among 128 576 participants experiencing chronic pain episodes, more than one-half of person-months of long-term opioid use occurred in women (52.7% of person-months among those with commercial insurance and 62.4% of person-months among MA beneficiaries). The median (interquartile range) age of the participants was 51 (41-58) years for patients in the commercial insurance group and 70 (61-77) years for those in the MA group. The mean (SE) extent of coprescription was 23.0% (0.18%) for the commercial insurance group and 25.7% (0.18%) for the MA group. The extent of coprescription decreased in the targeted guideline population-individuals with long-term opioid use-after the guideline release (postguideline slope, -0.95 percentages point per year [95% CI, -1.44 to -0.46 percentage points per year] for the commercial insurance group and -1.06 percentage points per year [95% CI, -1.49 to -0.63 percentage points per year] for the MA group). Nontargeted short-term episodes of opioid use were associated with no change or small declines in trend (for the MA group, postguideline slope of 0.47 percentage point per year [95% CI, 0.35-0.59 percentage point per year]; for the commercial insurance group, postguideline slope of -0.05 percentage point per year [95% CI, -0.12 to 0.02 percentage point per year]). High coprescribing intensity was seen, with 79.3% (95% CI, 78.9%-79.6%) of opioid prescription days in the commercial insurance group and 83.9% (95% CI, 83.7%-84.2%) in the MA group overlapping with benzodiazepines. There was no change in the intensity of coprescribing. Intensity of coprescription was higher when the same clinician prescribed opioids and benzodiazepines.
This study observed a reduction in the extent but not intensity of coprescribing of benzodiazepines for patients with long-term opioid use.
疾病预防控制中心在 2016 年的指南建议避免同时使用阿片类药物和苯二氮䓬类药物。
确定指南的发布是否与阿片类药物和苯二氮䓬类药物联合使用的变化有关。
设计、设置和参与者:这项回顾性队列研究使用了来自美国医疗保险和药房索赔全国数据库的数据,包括 3598322 名成年商业保险患者和 1299142 名 Medicare Advantage(MA)受益人,他们在研究期间(2014 年 1 月 1 日至 2018 年 3 月 31 日)没有癌症、镰状细胞病或临终关怀的近期病史。
重叠的阿片类药物和苯二氮䓬类药物处方。
联合处方的程度(有重叠处方天数的人月比例)和强度(处方阿片类药物时同时提供苯二氮䓬类药物的天数比例)。
在 4897464 名患者(使用了 1340 万人月的阿片类药物)中,独特的商业保险个体总数为 3598322 人(1974731 名女性[54.9%]),独特的 MA 受益人数为 1299142 人(770256 名女性[59.3%])。在 128576 名经历慢性疼痛发作的参与者中,超过一半的长期阿片类药物使用发生在女性(商业保险患者中有 52.7%的人月,MA 受益人的有 62.4%的人月)。参与者的中位数(四分位距)年龄为商业保险组 51(41-58)岁,MA 组 70(61-77)岁。商业保险组和 MA 组的联合处方程度的平均值(SE)分别为 23.0%(0.18%)和 25.7%(0.18%)。在指南发布后(商业保险组每年下降 0.95 个百分点[95%CI,每年 1.44 至 0.46 个百分点],MA 组每年下降 1.06 个百分点[95%CI,每年 1.49 至 0.63 个百分点]),长期阿片类药物使用者的目标指南人群的联合处方程度有所下降。短期非目标性阿片类药物使用的趋势没有变化或略有下降(MA 组为每年 0.47 个百分点[95%CI,每年 0.35 至 0.59 个百分点];商业保险组为每年 0.05 个百分点[95%CI,每年 0.12 至 0.02 个百分点])。高联合处方强度也可见,商业保险组中有 79.3%(95%CI,78.9%-79.6%)的阿片类药物处方日与苯二氮䓬类药物重叠,MA 组中有 83.9%(95%CI,83.7%-84.2%)的阿片类药物处方日与苯二氮䓬类药物重叠。联合处方的强度没有变化。当同一名临床医生同时开阿片类药物和苯二氮䓬类药物时,联合处方的强度更高。
本研究观察到长期使用阿片类药物的患者联合使用苯二氮䓬类药物的程度降低,但强度没有变化。