Academic Department of Radiation Oncology, Centre Oscar Lambret, Lille, France
CRIStAL UMR CNRS 9189, Lille University, Villeneuve-d'Ascq, France.
BMJ Open. 2019 Aug 2;9(8):e026666. doi: 10.1136/bmjopen-2018-026666.
Prostate cancer is the third most important cancer in terms of mortality in men. No standard local treatment exists for patients with an intraprostatic recurrence after radiotherapy. Stereotatic body radiotherapy (SBRT) could be a curative treatment for local recurrence. The phase I/II primary objective is the selection of the recommended dose for salvage-SBRT and to estimate the efficacy.
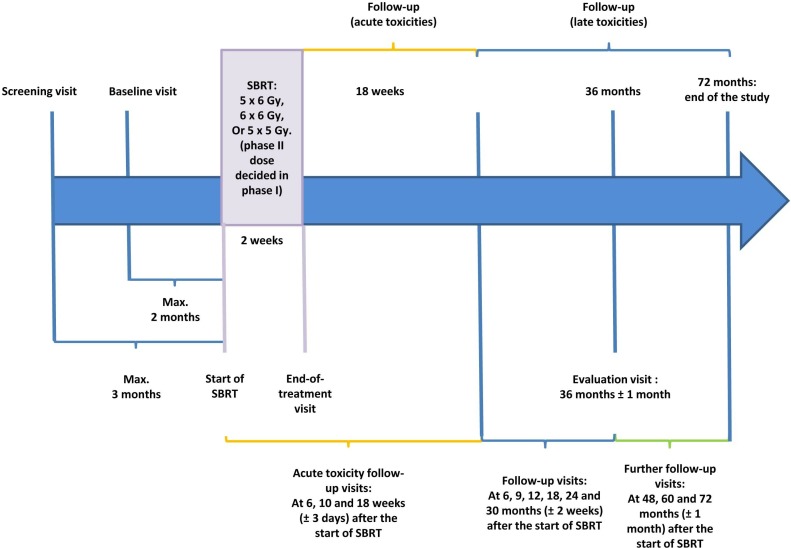
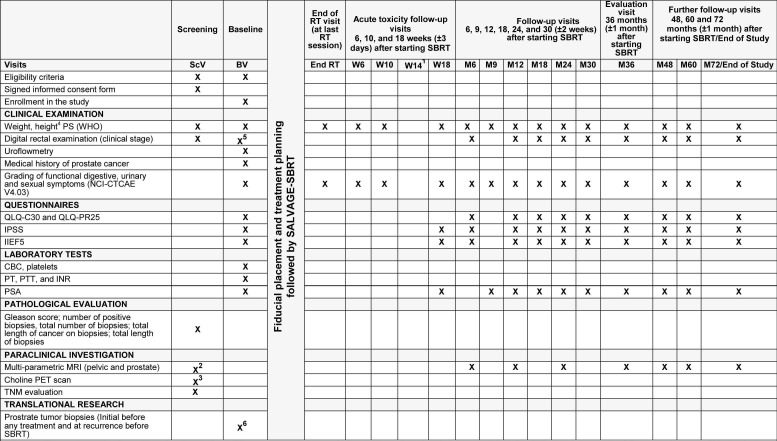
We plan to perform a multicentre prospective phase I/II study including at least 47 patients. Eligible patients are patients with biochemical recurrence occurring at least 2 years after external radiotherapy for prostatic adenocarcinoma by the Phoenix definition (prostate-specific antigen (PSA) nadir +2 ng/mL) and histologically proven intraprostatic recurrence only (stage T1-T2 on relapse, PSA level ≤10 ng/mL, PSA doubling time >10 months, absence of pelvic or metastatic recurrence proven by choline or PSMA positron emission tomography scan, and pelvic and prostatic assessment by multiparametric MRI). The phase I primary objective is the selection of the recommended dose for salvage-SBRT (5×6, 6×6 or 5×5 Gy) based on dose-limiting toxicity (DLT). The dose of salvage-SBRT will be selected using a time-to-event continual reassessment method based on DLT defined as grade ≥3 gastrointestinal or urinary toxicity or any other grade 4 adverse event. The phase II primary outcome is to estimate the efficacy of the salvage-SBRT in terms of biochemical relapse-free survival rate (Phoenix definition: increase in serum total PSA ≥2 ng/mL above the nadir). Phase II secondary outcomes are acute and late toxicities, quality of life, clinical progression-free survival defined as the time interval between the date of registration and the date of clinical progression or death irrespective of the cause.
The study has received ethical approval from the Ethics committee 'Ile-de-France III'. Academic dissemination will occur through publication and conference presentations.
NCT03438552.
前列腺癌是男性死亡人数排名第三的重要癌症。对于放射治疗后出现前列腺内复发的患者,尚无标准的局部治疗方法。立体定向体部放射治疗(SBRT)可能是局部复发的一种根治性治疗方法。I/II 期的主要目标是选择挽救性 SBRT 的推荐剂量,并评估疗效。
我们计划开展一项多中心前瞻性 I/II 期研究,纳入至少 47 例患者。合格患者为符合以下标准的患者:前列腺腺癌外照射治疗后至少 2 年出现生化复发(Phoenix 定义:前列腺特异性抗原(PSA)最低点+2ng/mL),且仅存在前列腺内复发(复发时分期为 T1-T2,PSA 水平≤10ng/mL,PSA 倍增时间>10 个月,通过胆碱或 PSMA 正电子发射断层扫描证实无盆腔或远处复发,多参数 MRI 评估盆腔和前列腺),组织学证实。I 期的主要目标是根据剂量限制毒性(DLT)选择挽救性 SBRT(5×6、6×6 或 5×5Gy)的推荐剂量。挽救性 SBRT 的剂量将使用基于 DLT 的时间事件连续再评估方法选择,DLT 定义为≥3 级胃肠道或泌尿系统毒性或任何其他 4 级不良事件。II 期的主要疗效终点是根据生化无复发生存率(Phoenix 定义:血清总 PSA 较最低点增加≥2ng/mL)评估挽救性 SBRT 的疗效。II 期次要终点是急性和晚期毒性、生活质量、临床无进展生存率(定义为登记日期和临床进展或死亡日期之间的时间间隔,无论原因如何)。
该研究已获得“法兰西岛 III 区”伦理委员会的批准。学术传播将通过发表文章和会议报告进行。
NCT03438552。