Institute of Pharmacology of Natural Products and Clinical Pharmacology, Ulm University, Ulm, Germany.
Institute of Transfusion Medicine, University of Ulm, Ulm, Germany.
Front Immunol. 2019 Jul 18;10:1639. doi: 10.3389/fimmu.2019.01639. eCollection 2019.
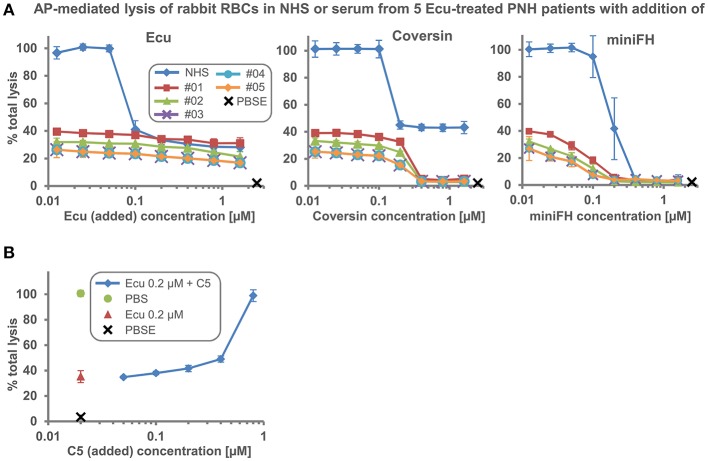
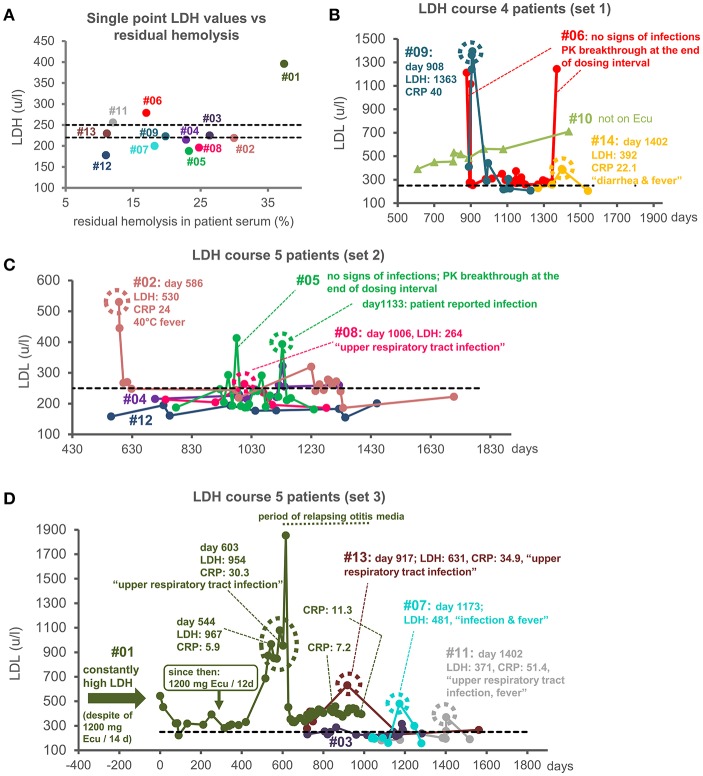
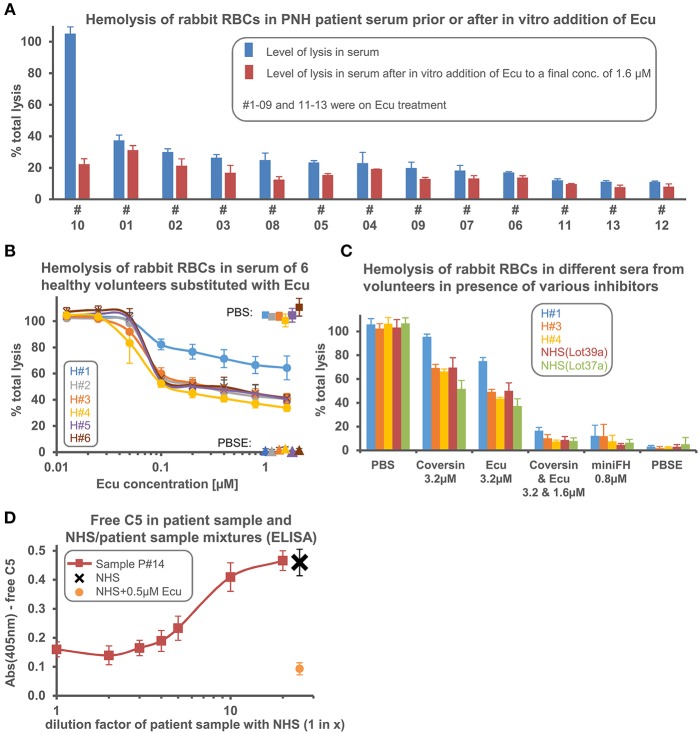
Eculizumab blocks the lytic complement pathway by inhibiting C5 and has become the standard of care for certain complement-mediated diseases. Previously, we have shown that strong complement activation overrides the C5 inhibition by Eculizumab, which accounts for residual terminal pathway activity. Here we show that the levels of residual hemolysis in assays differ markedly (up to 3.4-fold) across sera collected from different paroxysmal nocturnal hemoglobinuria (PNH) patients on Eculizumab treatment. This large variability of residual activity was also found in sera of healthy donors, thus cross-validating the findings in patients. While PNH patients with residual lytic activities of 11-30% exhibited hemolysis levels around the upper limit of normal (i.e., plasma LDH of ~250 u/L), as expected for PNH patients on Eculizumab therapy, we found sustained and markedly increased LDH levels of around 400 u/L for the patient with the highest residual activity of 37%. Furthermore, the clinical history of nine out of 14 PNH patients showed intravascular breakthrough hemolysis at the time of documented infections despite ample amounts of administered Eculizumab and/or experimentally determined excess over C5. The occurrence of extraordinary high levels of residual terminal pathway activity in PNH patients receiving Eculizumab is rare, but can impair the suppression of hemolysis. The commonly observed low levels of residual terminal pathway activity seen for most PNH patients can exacerbate during severe infections and, thus, can cause pharmacodynamic breakthrough hemolysis in PNH patients treated with Eculizumab.
依库珠单抗通过抑制 C5 阻断补体的裂解途径,已成为某些补体介导疾病的标准治疗方法。此前,我们已经表明,强烈的补体激活会抵消依库珠单抗对 C5 的抑制作用,从而导致末端途径活性残留。在这里,我们表明,在依库珠单抗治疗的不同阵发性睡眠性血红蛋白尿症(PNH)患者的血清中,残留溶血的水平差异显著(高达 3.4 倍)。这种残留活性的巨大变异性也在健康供体的血清中发现,从而验证了患者中的发现。虽然溶血活性残留为 11-30%的 PNH 患者的溶血水平接近正常值上限(即,血浆 LDH 约为 250u/L),正如依库珠单抗治疗的 PNH 患者预期的那样,但我们发现,在残留活性最高的患者(为 37%)中,LDH 水平持续显著升高至约 400u/L。此外,14 名 PNH 患者中有 9 名的临床病史显示,尽管给予了充足的依库珠单抗和/或实验确定的 C5 过量,但在有记录的感染时仍发生血管内溶血突破。在接受依库珠单抗治疗的 PNH 患者中,罕见出现残留末端途径活性异常高的情况,但会损害对溶血的抑制作用。大多数 PNH 患者观察到的残留末端途径活性的常见低水平,在严重感染期间可能会加剧,因此可能导致接受依库珠单抗治疗的 PNH 患者发生药效学突破溶血。