Institute of Clinical and Experimental Trauma Immunology, University Hospital of Ulm, Ulm, Germany.
Institute of Experimental and Clinical Pharmacology, Toxicology and Pharmacology of Natural Products, University of Ulm Medical Center, Ulm, Germany.
Blood Adv. 2023 Oct 24;7(20):6367-6380. doi: 10.1182/bloodadvances.2023010817.
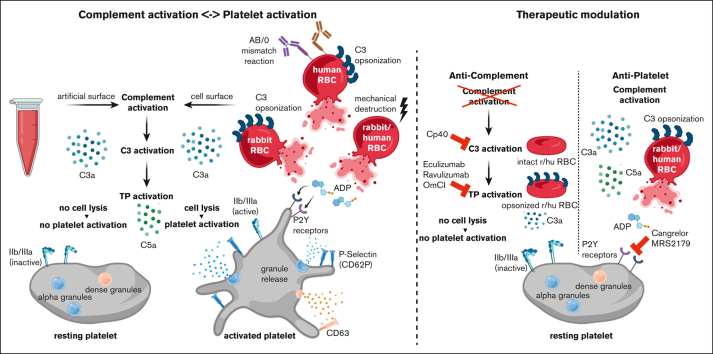
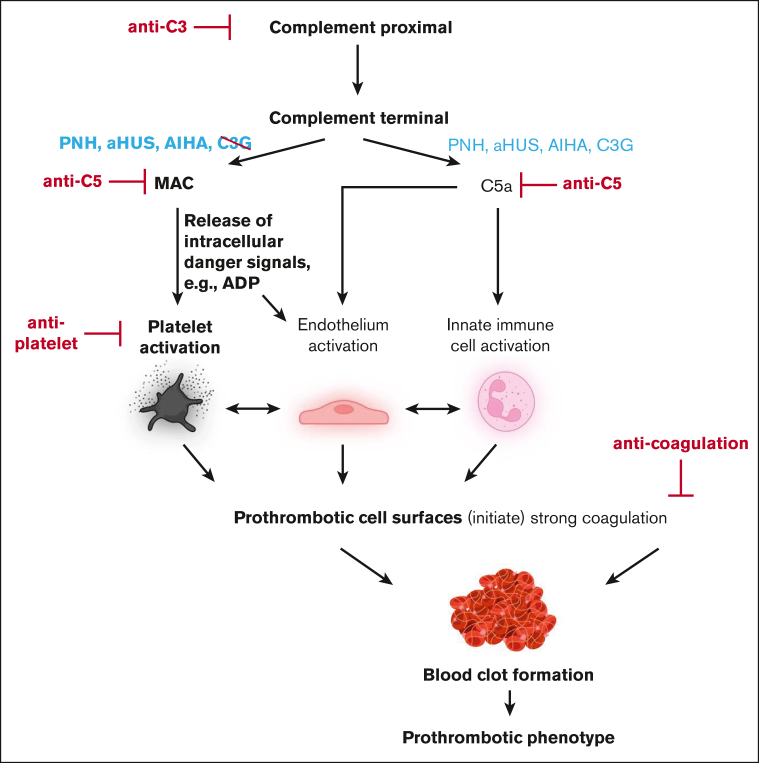
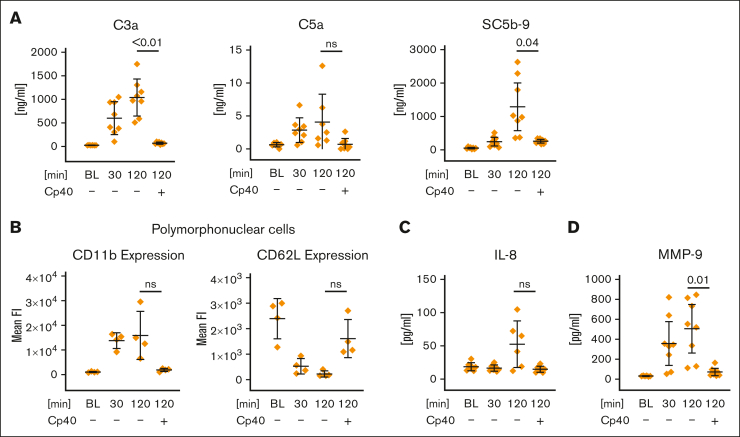
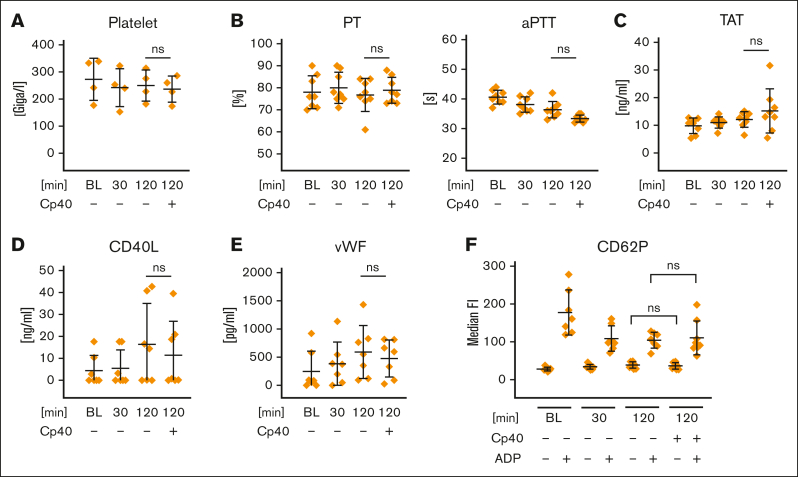
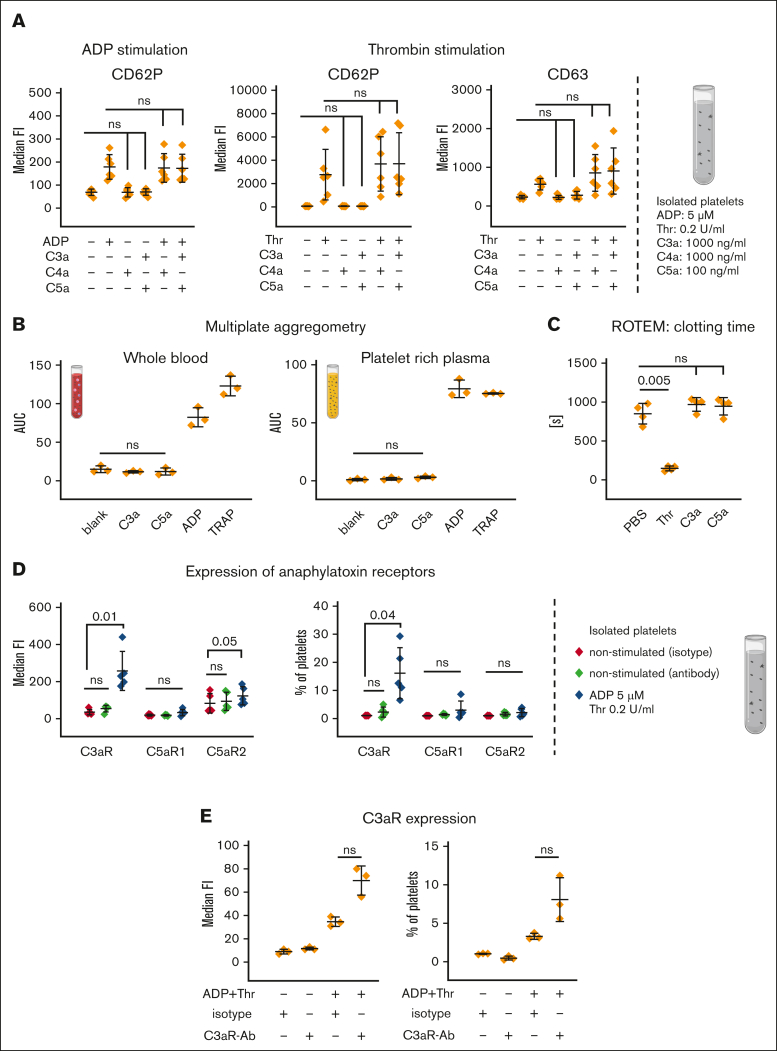
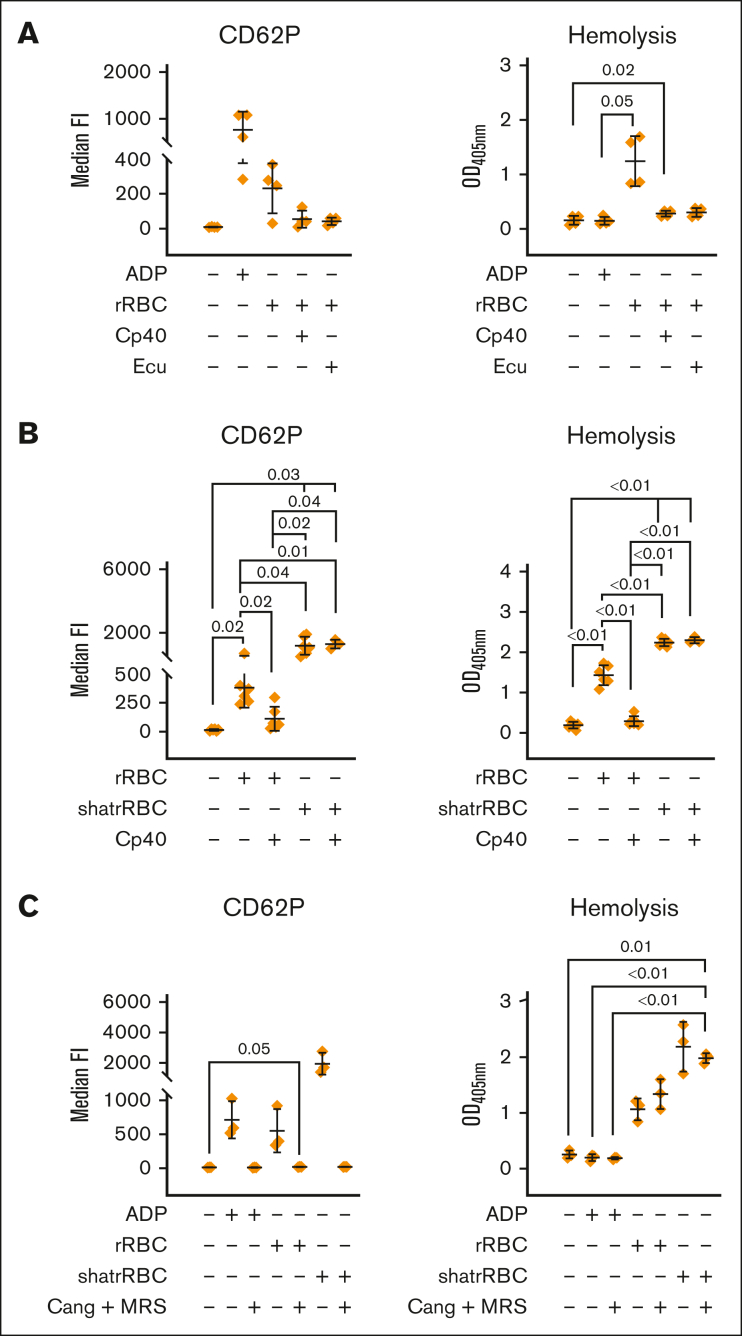
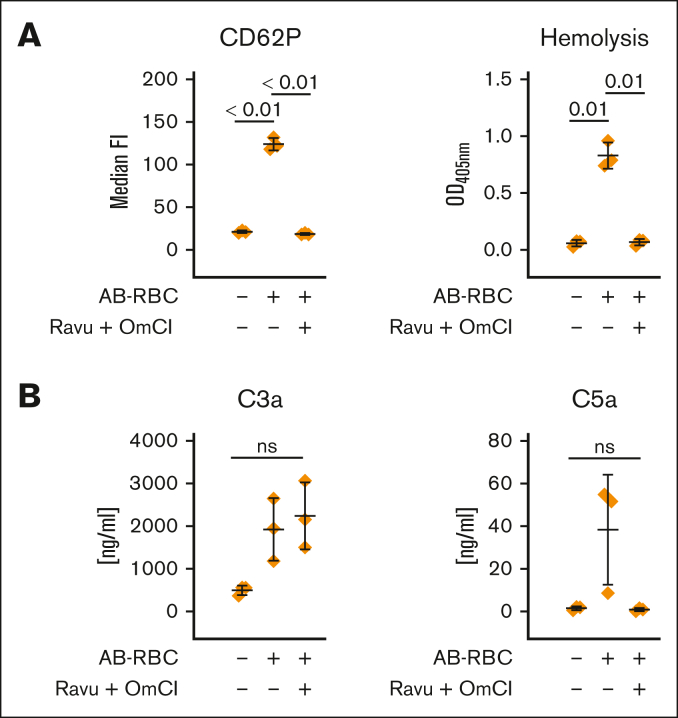
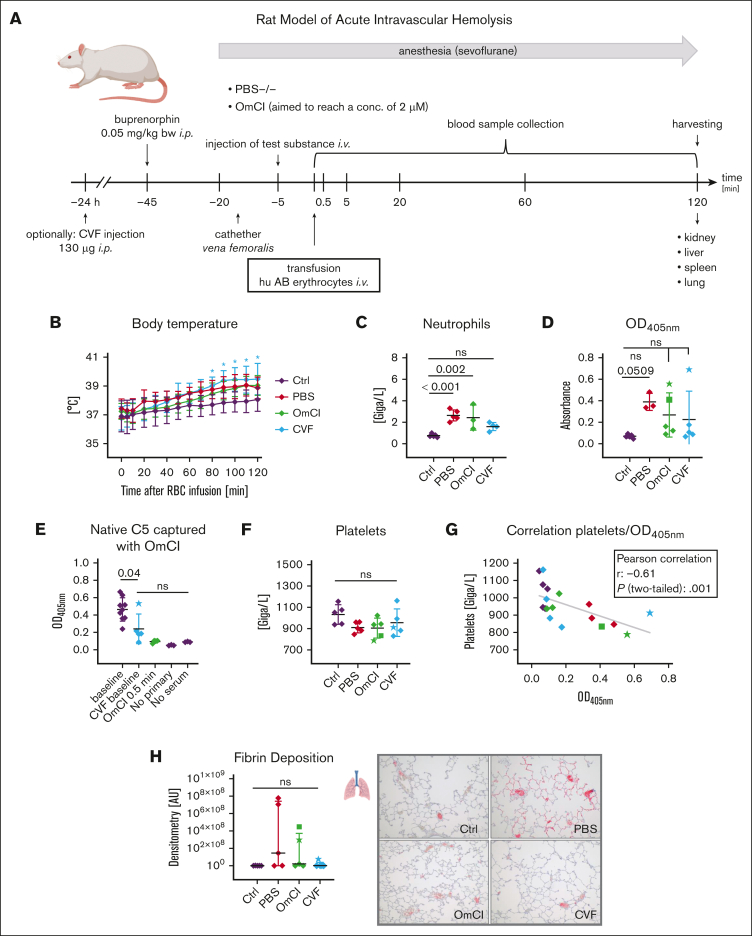
Complement activation in the diseases paroxysmal nocturnal hemoglobinuria (PNH) and atypical hemolytic uremic syndrome (aHUS) results in cytolysis and fatal thrombotic events, which are largely refractory to anticoagulation and/or antiplatelet therapy. Anticomplement therapy, however, efficiently prevents thrombotic events in PNH and aHUS, but the underlying mechanisms remain unresolved. We show that complement-mediated hemolysis in whole blood induces platelet activation similarly to activation by adenosine 5'-diphosphate (ADP). Blockage of C3 or C5 abolished platelet activation. We found that human platelets failed to respond functionally to the anaphylatoxins C3a and C5a. Instead, complement activation did lead to prothrombotic cell activation in the whole blood when membrane attack complex (MAC)-mediated cytolysis occurred. Consequently, we demonstrate that ADP receptor antagonists efficiently inhibited platelet activation, although full complement activation, which causes hemolysis, occurred. By using an established model of mismatched erythrocyte transfusions in rats, we crossvalidated these findings in vivo using the complement inhibitor OmCI and cobra venom factor. Consumptive complement activation in this animal model only led to a thrombotic phenotype when MAC-mediated cytolysis occurred. In conclusion, complement activation only induces substantial prothrombotic cell activation if terminal pathway activation culminates in MAC-mediated release of intracellular ADP. These results explain why anticomplement therapy efficiently prevents thromboembolisms without interfering negatively with hemostasis.
补体在阵发性夜间血红蛋白尿症(PNH)和非典型溶血尿毒症综合征(aHUS)中的激活导致细胞溶解和致命的血栓事件,这些事件在很大程度上对抗凝和/或抗血小板治疗有抗性。然而,抗补体治疗有效地预防了 PNH 和 aHUS 中的血栓事件,但潜在的机制仍未解决。我们表明,全血中的补体介导的溶血与由二磷酸腺苷(ADP)激活的血小板激活相似。阻断 C3 或 C5 可消除血小板激活。我们发现人类血小板无法对过敏毒素 C3a 和 C5a 产生功能性反应。相反,当膜攻击复合物(MAC)介导的细胞溶解发生时,补体激活确实会导致全血中的促血栓细胞激活。因此,我们证明 ADP 受体拮抗剂能够有效地抑制血小板激活,尽管发生了导致溶血的完全补体激活。通过使用大鼠不相容红细胞输血的既定模型,我们使用补体抑制剂 OmCI 和眼镜蛇毒液因子在体内对这些发现进行了交叉验证。在该动物模型中,只有当 MAC 介导的细胞溶解发生时,消耗性补体激活才会导致血栓表型。总之,如果终末途径的激活导致 MAC 介导的细胞内 ADP 释放,补体激活只会引起实质性的促血栓细胞激活。这些结果解释了为什么抗补体治疗能够有效地预防血栓栓塞,而不会对止血产生负面影响。