Montefiore Medical Center/Albert Einstein College of Medicine, 3300 Kossuth Ave, Bronx, NY, 10467, USA.
New York University School of Medicine, New York, NY, USA.
BMC Infect Dis. 2019 Aug 8;19(1):703. doi: 10.1186/s12879-019-4344-1.
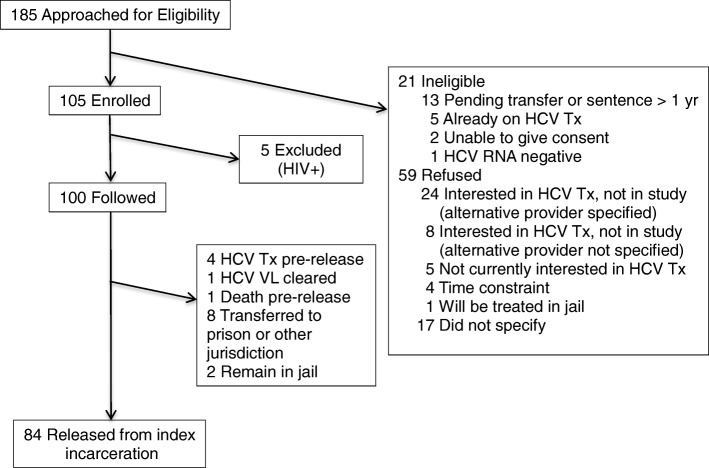
Hepatitis C virus (HCV) is a major public health problem in correctional settings. HCV treatment is often not possible in U.S. jails due to short lengths of stay. Linkage to care is crucial in these settings, but competing priorities complicate community healthcare engagement and retention after incarceration.
We conducted a single arm clinical trial of a combined transitional care coordination (TCC) and patient navigation intervention and assessed the linkage rate and factors associated with linkage to HCV care after incarceration.
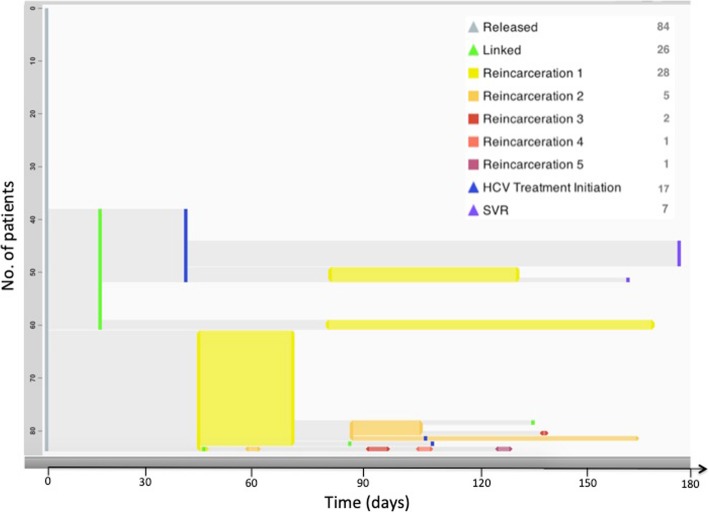
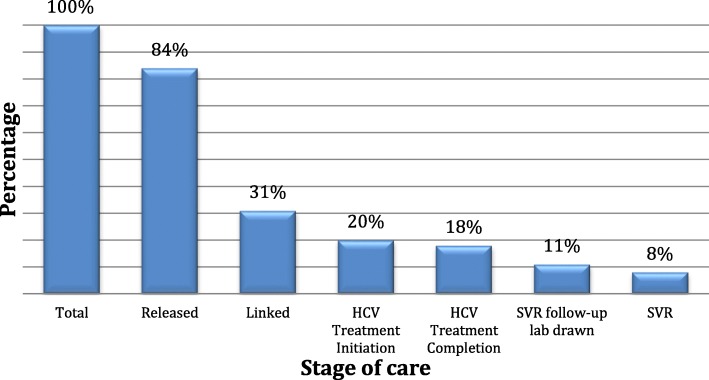
During the intervention, 84 participants returned to the community after their index incarceration. Most participants were male and Hispanic, with a history of mental illness and a mean age of 45 years. Of those who returned to the community, 26 (31%) linked to HCV care within a median of 20.5 days; 17 (20%) initiated HCV treatment, 15 (18%) completed treatment, 9 (11%) had a follow-up lab drawn to confirm sustained virologic response (SVR), and 7 (8%) had a documented SVR. Among those with follow-up labs the known SVR rate was (7/9) 78%. Expressing a preference to be linked to the participant's existing health system, being on methadone prior to incarceration, and feeling that family or a loved one were concerned about the participant's wellbeing were associated with linkage to HCV care. Reporting drinking alcohol to intoxication prior to incarceration was negatively associated with linkage to HCV care.
We demonstrate that an integrated strategy with combined TCC and patient navigation may be effective in achieving timely linkage to HCV care. Additional multicomponent interventions aimed at treatment of substance use disorders and increasing social support could lead to further improvement.
Clinicaltrials.gov NCT04036760 July 30th, 2019 (retrospectively registered).
丙型肝炎病毒(HCV)是监管场所的一个主要公共卫生问题。由于美国监狱关押时间短, HCV 治疗往往无法进行。在这些环境中,与医疗保健机构建立联系至关重要,但由于竞争因素,监禁后参与社区医疗保健服务并保持参与度存在困难。
我们开展了一项联合过渡性护理协调(TCC)和患者导航干预的单臂临床试验,并评估了监禁后与 HCV 护理建立联系的比例和相关因素。
在干预期间,84 名参与者在其索引监禁后返回社区。大多数参与者为男性和西班牙裔,有精神病史,平均年龄为 45 岁。在返回社区的人中,有 26 人(31%)在中位数为 20.5 天内与 HCV 护理建立联系;17 人(20%)开始 HCV 治疗,15 人(18%)完成治疗,9 人(11%)进行了后续实验室检查以确认持续病毒学应答(SVR),7 人(8%)有记录的 SVR。在进行了后续实验室检查的人中,已知 SVR 率为(7/9)78%。表达愿意与参与者现有的医疗系统建立联系、在监禁前服用美沙酮以及认为家人或亲人关心参与者的健康状况与 HCV 护理建立联系相关。在监禁前报告饮酒至醉酒与 HCV 护理建立联系呈负相关。
我们证明,结合 TCC 和患者导航的综合策略可能有助于及时与 HCV 护理建立联系。针对物质使用障碍治疗和增加社会支持的其他多成分干预措施可能会进一步改善这一结果。
Clinicaltrials.gov NCT04036760 2019 年 7 月 30 日(回顾性注册)。