Department of oncology, The second affiliated hospital of Nanchang University, Jiangxi province, Nanchang, 330006, China.
Jiangxi key laboratory of clinical translational cancer research, The second affiliated hospital of Nanchang University, Jiangxi province, Nanchang, 330006, China.
BMC Cancer. 2019 Aug 9;19(1):793. doi: 10.1186/s12885-019-6005-6.
The treatment strategy for brain metastasis (BM) in patients with epidermal growth factor receptor (EGFR) -mutant lung adenocarcinoma (LAC) remains controversial. In the present study, we compared the efficacy of brain radiotherapy (RT) in combination with tyrosine kinase inhibitors (TKIs) and TKIs alone for advanced LAC patients with EGFR mutations and BM.
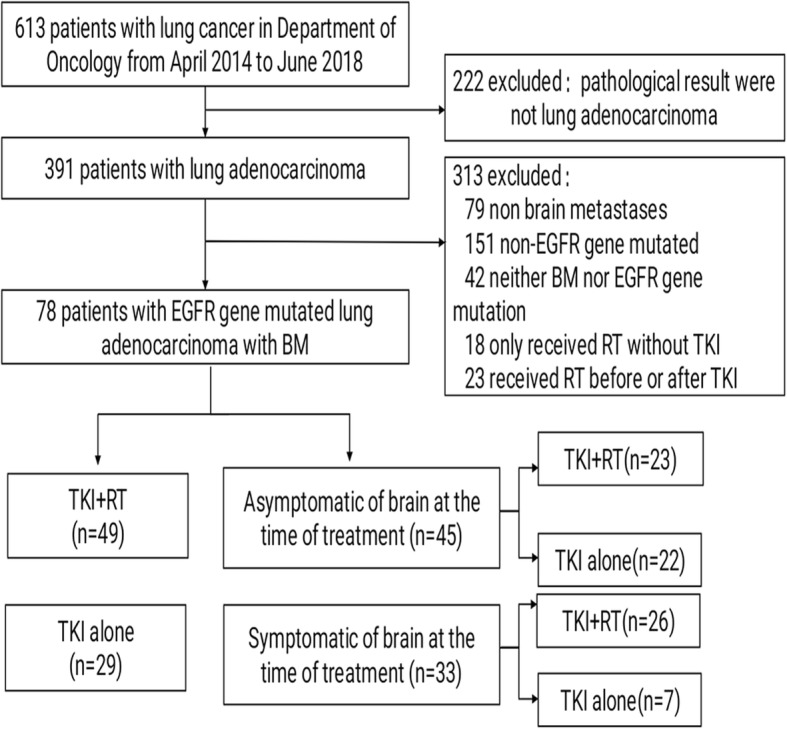
We retrospectively studied 78 patients diagnosed with EGFR-mutant LAC who developed BM. These patients were divided into two groups: 49 patients in the combination treatment group who received brain RT in combination with EGFR-TKIs (including 23 patients with asymptomatic BM before RT); 29 patients in the TKI group who received EGFR-TKI targeted therapy alone (including 22 patients with asymptomatic BM before TKI treatment).
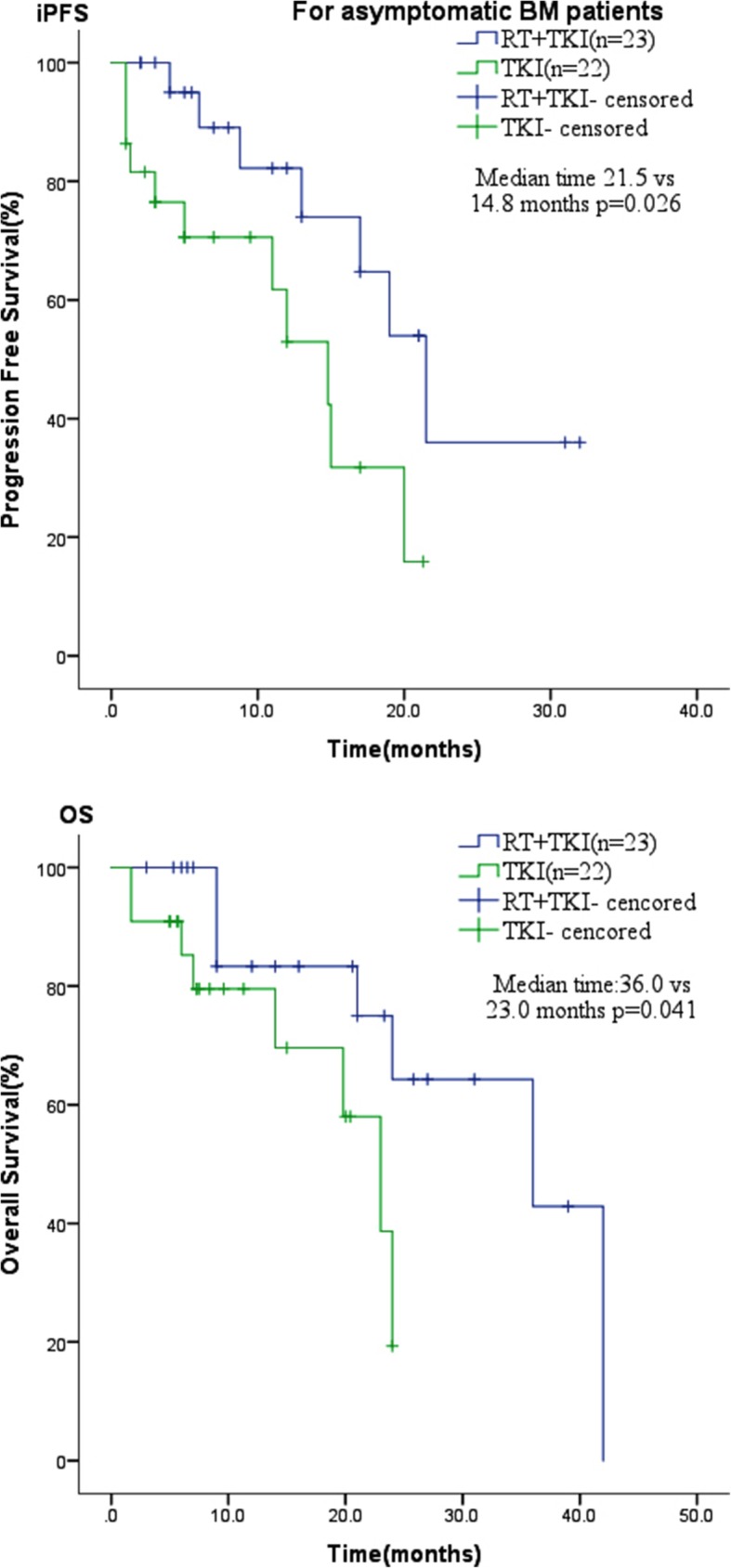
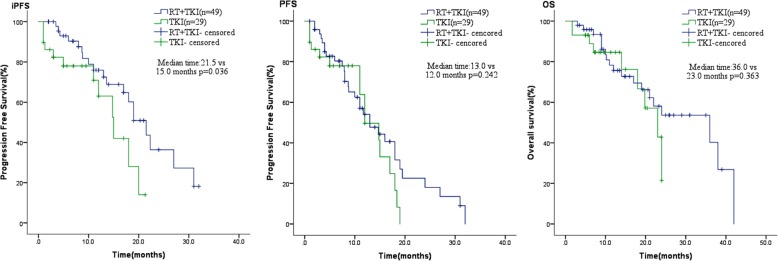
The median intracranial progression-free survival (iPFS) of the combination treatment group was longer than that of the TKI alone group (21.5 vs. 15 months; P = 0.036). However, there were no significant differences in median progression-free survival (PFS, 12 vs. 13 months; P = 0.242) and median overall survival (mOS, 36 vs. 23 months; P = 0.363) between the two groups. Further analysis of asymptomatic BM showed that both the median iPFS and the mOS of the combination treatment group were significantly longer than for the TKI alone group (iPFS, 21.5 vs. 14.8 months, P = 0.026; mOS, 36 vs. 23 months, P = 0.041). Cox multivariate regression analysis found no independent adverse predictors of iPFS in all patients.
The synchronous combination of brain RT and TKIs was superior to EGFR-TKIs alone for EGFR-mutant LAC patients with BM. The combination treatment group exhibited longer iPFS, while the PFS and OS were not significantly different between the two groups. In addition, the combination treatment could result in better iPFS and OS in those with asymptomatic BM. Therefore, addition of brain RT was useful for intracranial metastatic lesions.
表皮生长因子受体(EGFR)突变型肺腺癌(LAC)患者脑转移(BM)的治疗策略仍存在争议。本研究比较了脑放疗(RT)联合酪氨酸激酶抑制剂(TKI)与单独 TKI 治疗 EGFR 突变型 LAC 伴 BM 患者的疗效。
我们回顾性研究了 78 例诊断为 EGFR 突变型 LAC 并发生 BM 的患者。这些患者分为两组:49 例联合治疗组患者在 RT 时联合 EGFR-TKIs(包括 23 例 RT 前无症状 BM);29 例 TKI 组患者仅接受 EGFR-TKI 靶向治疗(包括 22 例 TKI 治疗前无症状 BM)。
联合治疗组患者的中位颅内无进展生存期(iPFS)长于 TKI 单药组(21.5 与 15 个月;P=0.036)。但两组患者的中位无进展生存期(PFS,12 与 13 个月;P=0.242)和中位总生存期(mOS,36 与 23 个月;P=0.363)均无显著差异。进一步分析无症状 BM 显示,联合治疗组的中位 iPFS 和 mOS 均显著长于 TKI 单药组(iPFS,21.5 与 14.8 个月,P=0.026;mOS,36 与 23 个月,P=0.041)。Cox 多因素回归分析显示,所有患者的 iPFS 均无独立的不良预测因素。
对于 EGFR 突变型 LAC 伴 BM 患者,脑 RT 与 TKI 的同步联合应用优于单独应用 EGFR-TKIs。联合治疗组患者的 iPFS 更长,而两组患者的 PFS 和 OS 无显著差异。此外,对于无症状 BM 患者,联合治疗可获得更好的 iPFS 和 OS。因此,脑 RT 有助于颅内转移病灶。