Department of Cardiovascular Sciences, University of Leicester, National Institute for Health Research (NIHR) Leicester Biomedical Research Centre, Leicester, UK.
Aintree University Hospital, Liverpool, UK.
Int J Cardiovasc Imaging. 2020 Jan;36(1):101-110. doi: 10.1007/s10554-019-01684-9. Epub 2019 Aug 10.
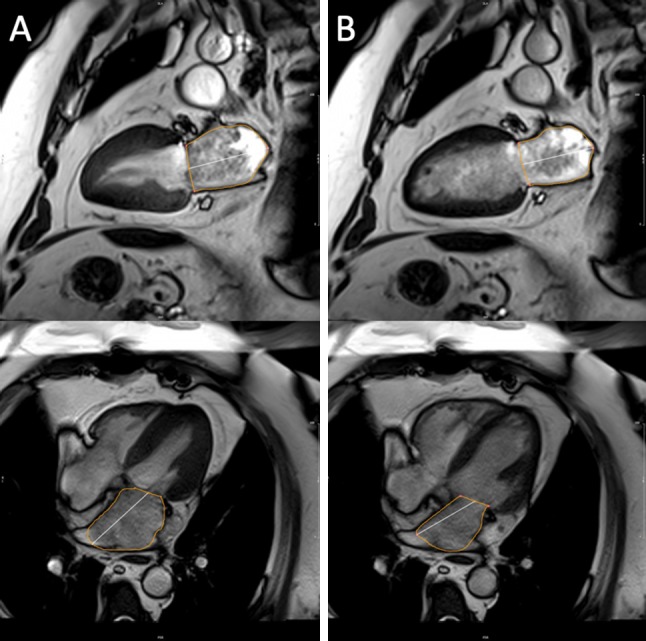
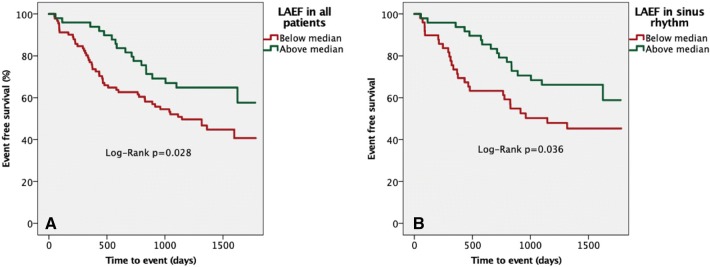
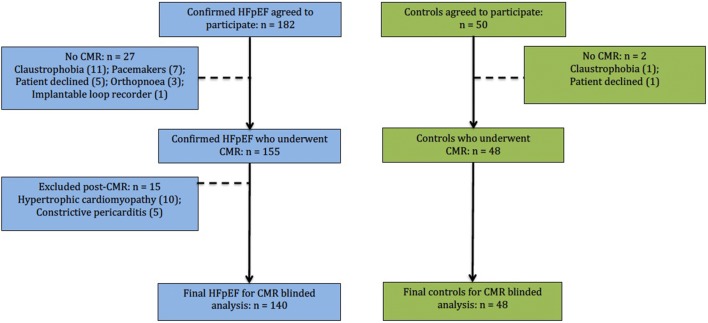
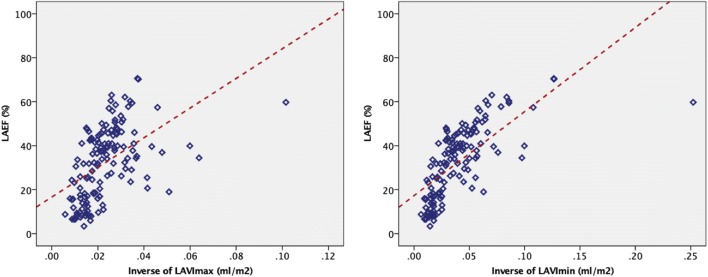
The aim of this study was to determine whether left atrial ejection fraction (LAEF) quantified with cardiovascular magnetic resonance (CMR) was different between heart failure with preserved ejection fraction (HFpEF) and controls, and its relation to prognosis. As part of our single-centre, prospective, observational study, 188 subjects (HFpEF n = 140, controls n = 48) underwent phenotyping with contrast-enhanced CMR, transthoracic echocardiography, blood sampling and six-minute walk testing. LAEF was calculated using the biplane method. Atrial fibrillation (AF) was present in 43 (31%) of HFpEF subjects. Overall, LAEF (%) was lower in HFpEF patients inclusive of AF (32 ± 16) or those in sinus rhythm alone (41 ± 12) compared to controls (51 ± 11), p < 0.0001. LAEF correlated inversely with maximal and minimal left atrial volumes indexed (r = - 0.602, r = - 0.762), and plasma N-terminal pro-atrial natriuretic peptide (r = - 0.367); p < 0.0001. During median follow-up (1429 days), there were 67 composite events of all-cause death or hospitalization for heart failure (22 deaths, 45 HF hospitalizations) in HFpEF. Lower LAEF (below median) was associated with an increased risk of composite endpoints (Log-Rank: all p = 0.028; sinus p = 0.036). In multivariable Cox regression analysis, LAEF (adjusted hazard ratio [HR] 0.767, 95% confidence interval [CI] 0.591-0.996; p = 0.047) and indexed extracellular volume (HR 1.422, CI 1.015-1.992; p = 0.041) were the only parameters that remained significant when added to a base prognostic model comprising age, prior HF hospitalization, diastolic blood pressure, lung disease, NYHA, six-minute-walk-test-distance, haemoglobin, creatinine and B-type natriuretic peptide. CMR-derived LAEF is lower in HFpEF compared to healthy controls and is a strong prognostic biomarker.
本研究旨在确定左心房射血分数(LAEF)是否存在差异,并用心血管磁共振(CMR)量化心力衰竭伴射血分数保留(HFpEF)和对照组之间的差异,及其与预后的关系。作为我们单中心前瞻性观察研究的一部分,188 名受试者(HFpEF n=140,对照组 n=48)接受了对比增强 CMR、经胸超声心动图、血液采样和 6 分钟步行测试的表型分析。使用双平面法计算 LAEF。在 HFpEF 受试者中,43 例(31%)存在心房颤动(AF)。总的来说,包含 AF(32±16)或窦性心律(41±12)的 HFpEF 患者的 LAEF(%)明显低于对照组(51±11),p<0.0001。LAEF 与最大和最小左心房容积指数呈负相关(r=-0.602,r=-0.762),与血浆 N-末端脑钠肽前体(r=-0.367)呈负相关;p<0.0001。在中位随访期间(1429 天),HFpEF 中有 67 例全因死亡或心力衰竭住院的复合终点事件(22 例死亡,45 例心力衰竭住院)。较低的 LAEF(低于中位数)与复合终点的风险增加相关(对数秩检验:均 p=0.028;窦性心律 p=0.036)。在多变量 Cox 回归分析中,LAEF(调整后的危险比[HR]0.767,95%置信区间[CI]0.591-0.996;p=0.047)和细胞外容积指数(HR 1.422,CI 1.015-1.992;p=0.041)是在加入包含年龄、HF 住院史、舒张期血压、肺部疾病、NYHA、6 分钟步行试验距离、血红蛋白、肌酐和 B 型利钠肽的基本预后模型后,唯一具有统计学意义的参数。与健康对照组相比,HFpEF 中的 CMR 衍生 LAEF 较低,是一种强大的预后生物标志物。