Departments of Obstetrics, Gynecology and Women's Health, Laboratory Medicine and Pathology, and Surgery, University of Minnesota School of Medicine, the Department of Biostatistics and Bioinformatics Core, Masonic Cancer Center, University of Minnesota, and the University of Minnesota School of Medicine, Minneapolis, Minnesota.
Obstet Gynecol. 2019 Sep;134(3):520-526. doi: 10.1097/AOG.0000000000003421.
To evaluate health care provider adherence to the surgical protocol endorsed by the National Comprehensive Cancer Network and the American College of Obstetricians and Gynecologists at the time of risk-reducing salpingo-oophorectomy and compare adherence between gynecologic oncologists and obstetrician-gynecologists (ob-gyns).
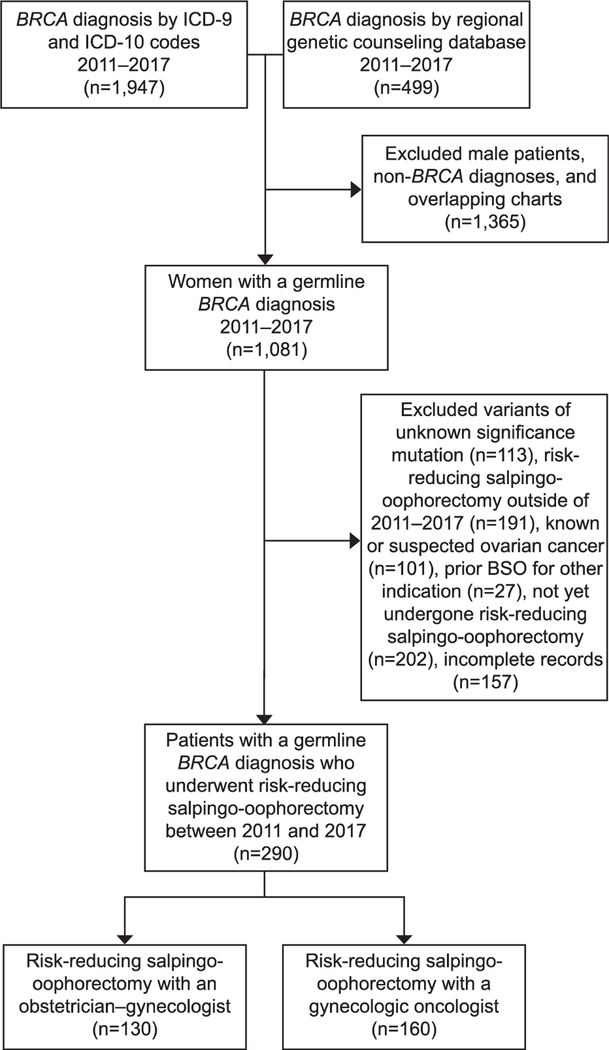
In this multicenter retrospective cohort study, women were included if they had a pathogenic BRCA mutation and underwent risk-reducing salpingo-oophorectomy between 2011 and 2017. Adherence was defined as completing all of the following: collection of washings, complete resection of the fallopian tube, and performing the Sectioning and Extensively Examining the Fimbriated End (SEE-FIM) pathologic protocol.
Of 290 patients who met inclusion criteria, 160 patients were treated by 18 gynecologic oncologists and 130 patients by 75 ob-gyns. Surgery was performed at 10 different hospitals throughout a single metropolitan area. Demographic and clinical characteristics were similar between groups. Overall, 199 cases (69%) were adherent to the surgical protocol. Gynecologic oncologists were more than twice as likely to fully adhere to the full surgical protocol as ob-gyns (91% vs 41%, P<.01). Specifically, gynecologic oncologists were more likely to resect the entire tube (99% vs 95%, P=.03), to have followed the SEE-FIM protocol (98% vs 82%, P<.01), and collect washings (94% vs 49%, P<.01). Complication rates did not differ between groups. Occult neoplasia was diagnosed in 11 patients (3.8%). The incidence of occult neoplasia was 6.3% in gynecologic oncology patients and 0.8% in obstetrics and gynecology patients (P=.03).
Despite clear surgical guidelines, only two thirds of all health care providers were fully adherent to guidelines. Gynecologic oncologists were more likely to follow surgical guidelines compared with general ob-gyns and more likely to diagnose occult neoplasia despite similar patient populations. Rates of risk-reducing surgery will likely continue to increase as genetic testing becomes more widespread, highlighting the importance of health care provider education for this procedure. Centralized care or referral to subspecialists for risk-reducing salpingo-oophorectomy may be warranted.
评估医疗保健提供者在实施降低风险的输卵管卵巢切除术时对美国国家综合癌症网络和美国妇产科医师学会推荐的手术方案的依从性,并比较妇科肿瘤学家和妇产科医生(ob-gyns)之间的依从性。
本多中心回顾性队列研究纳入了 2011 年至 2017 年间患有致病性 BRCA 突变并接受降低风险的输卵管卵巢切除术的女性。依从性定义为完成以下所有操作:收集冲洗液、完全切除输卵管,以及执行 Sectioning and Extensively Examining the Fimbriated End (SEE-FIM) 病理方案。
在符合纳入标准的 290 名患者中,160 名患者由 18 名妇科肿瘤学家治疗,130 名患者由 75 名妇产科医生治疗。手术在单个大都市地区的 10 家不同医院进行。两组患者的人口统计学和临床特征相似。总体而言,199 例(69%)符合手术方案。妇科肿瘤学家完全遵循完整手术方案的可能性是妇产科医生的两倍多(91%比 41%,P<.01)。具体而言,妇科肿瘤学家更有可能切除整个输卵管(99%比 95%,P=.03),遵循 SEE-FIM 方案(98%比 82%,P<.01),以及收集冲洗液(94%比 49%,P<.01)。两组并发症发生率无差异。11 名患者(3.8%)诊断为隐匿性肿瘤。妇科肿瘤学患者的隐匿性肿瘤发生率为 6.3%,妇产科患者为 0.8%(P=.03)。
尽管有明确的手术指南,但只有三分之二的医疗保健提供者完全遵循指南。与普通妇产科医生相比,妇科肿瘤学家更有可能遵循手术指南,尽管患者人群相似,但更有可能诊断隐匿性肿瘤。随着基因检测的广泛应用,降低风险的手术率可能会继续增加,这凸显了该手术的医疗保健提供者教育的重要性。可能需要集中护理或转介给专家进行降低风险的输卵管卵巢切除术。