Department of General, Visceral, Thoracic, Transplant and Pediatric Surgery, University Hospital of Giessen, Rudolf-Buchheim Strasse 7, D-35392, Giessen, Germany.
Department of Anesthesiology, Heidelberg University Hospital, Im Neuenheimer Feld 110, D-69120, Heidelberg, Germany.
Sci Rep. 2019 Aug 14;9(1):11856. doi: 10.1038/s41598-019-48234-w.
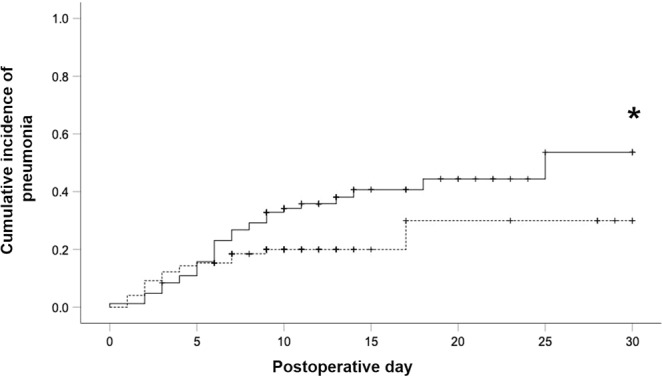
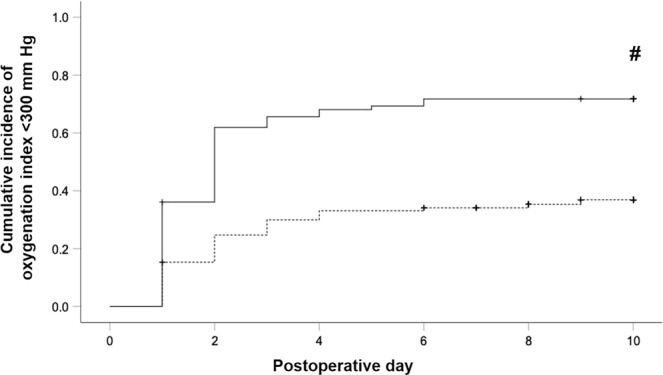
Pulmonary complications and a poor clinical outcome are common in response to transthoracic esophagectomy, but their etiology is not well understood. Clinical observation suggests that patients undergoing pulmonary resection, a surgical intervention with similarities to the thoracic part of esophagectomy, fare much better, but this has not been investigated in detail. A retrospective single-center analysis of 181 consecutive patients after right-sided thoracotomy for either Ivor Lewis esophagectomy (n = 83) or major pulmonary resection (n = 98) was performed. An oxygenation index <300 mm Hg was used to indicate respiratory impairment. When starting surgery, respiratory impairment was seen more frequently in patients undergoing major pulmonary resection compared to esophagectomy patients (p = 0.009). On postoperative days one to ten, however, esophagectomy caused higher rates of respiratory impairment (p < 0.05) resulting in a higher cumulative incidence of postoperative respiratory impairment for patients after esophagectomy (p < 0.001). Accordingly, esophagectomy patients were characterized by longer ventilation times (p < 0.0001), intensive care unit and total postoperative hospital stays (both p < 0.0001). In conclusion, the postoperative clinical course including respiratory impairment after Ivor Lewis esophagectomy is significantly worse than that after major pulmonary resection. A detailed investigation of the underlying causes is required to improve the outcome of esophagectomy.
经胸食管切除术常伴有肺部并发症和不良临床转归,但其病因尚未完全明确。临床观察表明,接受肺切除术(一种与食管切除术的胸部部分相似的手术干预)的患者预后要好得多,但这尚未得到详细研究。对 181 例因右侧开胸行 Ivor Lewis 食管切除术(n=83)或大肺切除术(n=98)的连续患者进行了回顾性单中心分析。使用氧合指数 <300 mm Hg 来表示呼吸受损。当开始手术时,与食管切除术患者相比,大肺切除术患者更常出现呼吸受损(p=0.009)。然而,在术后第 1 至 10 天,食管切除术导致更高的呼吸受损发生率(p<0.05),导致食管切除术患者术后呼吸受损的累积发生率更高(p<0.001)。因此,食管切除术患者的通气时间更长(p<0.0001)、重症监护病房和总术后住院时间更长(均 p<0.0001)。总之,Ivor Lewis 食管切除术的术后临床过程,包括呼吸受损,明显比大肺切除术更差。需要对潜在原因进行详细调查,以改善食管切除术的结局。