Clinton Health Access Initiative, Lusaka, Zambia.
Clinton Health Access Initiative, Boston, MA, USA.
Trials. 2019 Aug 15;20(1):505. doi: 10.1186/s13063-019-3617-8.
Public health systems in resource-constrained settings have a critical role to play in the elimination of HIV transmission but are often financially constrained. This study is an evaluation of a mother-infant-pair model called "Umoyo," which was designed to be low cost and scalable in a public health system. Facilities with the Umoyo model dedicate a clinic day to provide services to only HIV-exposed infants (HEIs) and their mothers. Such models are in operation with reported success in Zambia but have not been rigorously tested. This work establishes whether the Umoyo model would improve 12-month retention of HEIs.
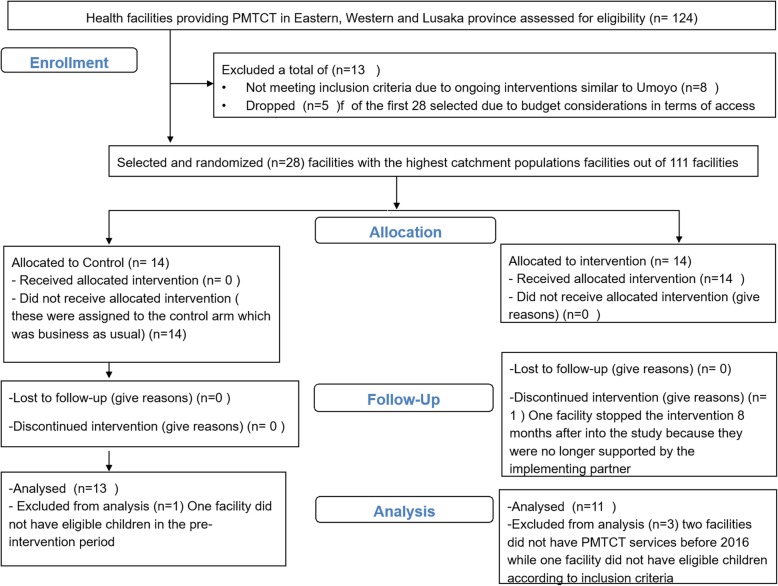
A cluster randomized trial including 28 facilities was conducted across two provinces of Zambia to investigate the impact on 12-month retention of HEIs in care. These facilities were offering Prevention of Mother-to-Child-Transmission (PMTCT) services and supported by the same implementing partner. Randomization was achieved by use of the covariate-constrained optimization technique. Secondary outcomes included the impact of Umoyo clinics on social support and perceived HIV stigma among mothers. For each of the outcomes, a difference-in-difference analysis was conducted at the facility level using the unweighted t test.
From 13 control (12-month retention at endline: 45%) and 11 intervention facilities (12-month retention at endline: 33%), it was found that Umoyo clinics had no impact on 12-month retention of HEIs in the t test (- 11%; 99% CI - 40.1%, 17.2%). Regarding social support and stigma, the un-weighted t test showed no impact though sensitivity tests showed that Umoyo had an impact on increasing social support (0.31; 99% CI 0.08, 0.54) and reducing perceived stigma from health care workers (- 0.27; 99% CI - 0.46, - 0.08).
The Umoyo approach of having a dedicated clinic day for HEIs and their mothers did not improve retention of HEIs though there are indications that it can increase social support among mothers and reduce stigma. Without further support to the underlying health system, based on the evidence generated through this evaluation, the Umoyo clinic day approach on its own is not considered an effective intervention to increase retention of HIV-exposed infants.
Pan African Clinical Trial Registry, ID: PACTR201702001970148 . Prospectively registered on 13 January 2017.
资源有限环境下的公共卫生系统在消除 HIV 传播方面发挥着至关重要的作用,但往往受到资金限制。本研究评估了一种名为“Umoyo”的母婴配对模式,该模式旨在以低成本和可扩展的方式在公共卫生系统中运行。采用“Umoyo”模式的机构专门划出一天的门诊时间,只为 HIV 暴露婴儿(HEI)及其母亲提供服务。这种模式在赞比亚已投入使用,并取得了报告中的成功,但尚未经过严格测试。本研究旨在确定“Umoyo”模式是否能够提高 HEI 患儿 12 个月的保留率。
本研究在赞比亚的两个省开展了一项包括 28 个机构的群组随机试验,以调查该模式对 12 个月内 HEI 患儿护理保留率的影响。这些机构正在提供预防母婴传播(PMTCT)服务,并由同一实施合作伙伴提供支持。通过使用协变量约束优化技术实现随机分组。次要结果包括“Umoyo”门诊对母亲社会支持和感知 HIV 耻辱感的影响。对于每个结果,在机构层面使用未加权 t 检验进行差异分析。
在 13 个对照组(12 个月时的保留率为 45%)和 11 个干预组(12 个月时的保留率为 33%)中,“Umoyo”门诊并未对 HEI 患儿 12 个月的保留率产生影响(-11%;99%置信区间-40.1%,17.2%)。在社会支持和耻辱感方面,未加权 t 检验未显示出影响,但敏感性测试表明“Umoyo”模式可增加母亲的社会支持(0.31;99%置信区间 0.08,0.54)并降低医护人员的感知耻辱感(-0.27;99%置信区间-0.46,-0.08)。
虽然有迹象表明,“Umoyo”模式为 HEI 及其母亲设立专门的门诊日可以增加母亲的社会支持并降低耻辱感,但该模式并不能提高 HEI 患儿的保留率。根据这项评估所产生的证据,如果没有对基本卫生系统的进一步支持,那么仅依靠“Umoyo”门诊日方法本身,并不被认为是提高 HIV 暴露婴儿保留率的有效干预措施。
泛非临床研究注册处,编号:PACTR201702001970148。于 2017 年 1 月 13 日前瞻性注册。