Departments of Medicine, Milton S. Hershey Medical Center, Pennsylvania State University, Hershey, PA.
Department of Anesthesia, Milton S. Hershey Medical Center, Pennsylvania State University, Hershey, PA.
Liver Transpl. 2019 Dec;25(12):1747-1755. doi: 10.1002/lt.25630. Epub 2019 Sep 19.
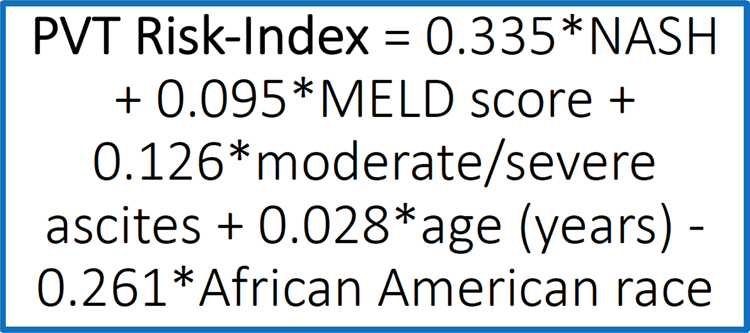
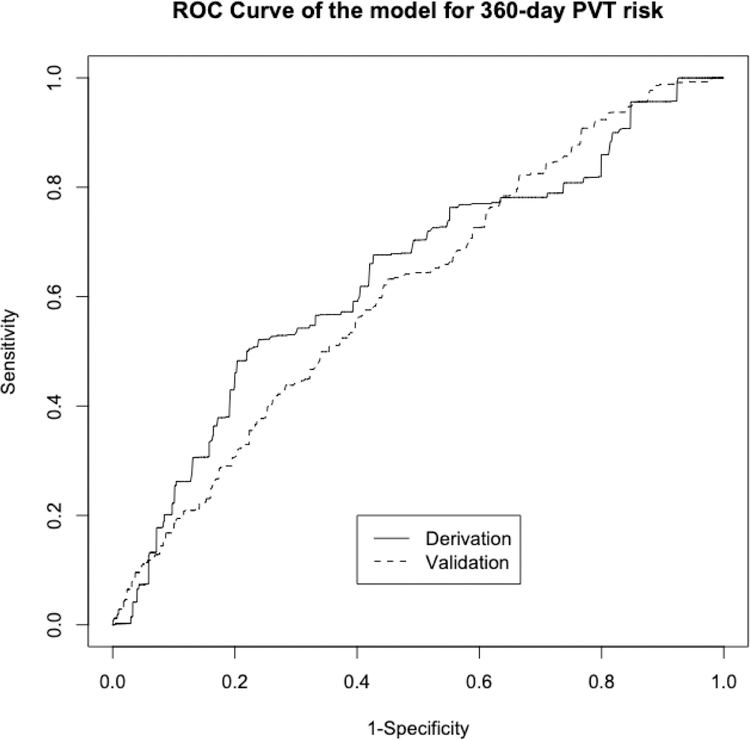
Portal vein thrombosis (PVT) is associated with inferior pretransplantation and posttransplantation outcomes. We aimed to create a predictive model to risk stratify transplant candidates for PVT. Data on adult transplants in the United States during the Model for End-Stage Liver Disease (MELD) era through September 2016 were reviewed. We constructed and validated a scoring system composed of routine, readily available clinical information to predict the development of incident PVT at 12 months from transplantation listing. A total of 66,568 liver transplant candidates were dichotomized into 2 groups to construct (n = 34,751) and validate (n = 31,817) a scoring system. In general, the derivation and validation cohorts were clinically similar. Although nonalcoholic steatohepatitis was a significant predictor of incident PVT (hazard ratio, 1.29; 95% confidence interval, 1.08-1.54; P < 0.001), age, MELD score, and moderate-to-severe ascites were also associated with increased risk. African American race was associated with decreased risk. A scoring system (PVT risk index [RI]) of these 5 variables had an area under the curve of 0.71 and 0.70 in both derivation and validation cohorts, respectively. By applying the low cutoff score of 2.6, incident PVT could be accurately excluded (negative predictive value 94%). Using the high cutoff score of 4.6 (positive predictive value 85%), PVT could be diagnosed with high accuracy. The PVT-RI predicts which candidates awaiting lifesaving liver transplantation will and will not develop future PVT. Although this scoring system will require prospective validation, it provides a powerful new tool for the clinician when risk stratifying cirrhosis patients prior to liver transplantation for future PVT development.
门静脉血栓形成(PVT)与肝移植前和移植后预后不良有关。我们旨在建立一个预测模型,对 PVT 移植候选者进行风险分层。对美国在终末期肝病模型(MELD)时代期间(截至 2016 年 9 月)的成人肝移植数据进行了回顾。我们构建并验证了一个评分系统,该系统由常规、易于获得的临床信息组成,用于预测从移植登记到 12 个月时发生 PVT 的情况。总共将 66568 名肝移植候选者分为两组,分别用于构建(n=34751)和验证(n=31817)评分系统。一般来说,推导和验证队列在临床上相似。尽管非酒精性脂肪性肝炎是发生 PVT 的重要预测指标(危险比,1.29;95%置信区间,1.08-1.54;P<0.001),但年龄、MELD 评分和中重度腹水也与风险增加相关。非裔美国人种族与风险降低相关。这 5 个变量的评分系统(PVT 风险指数[RI])在推导和验证队列中的曲线下面积分别为 0.71 和 0.70。通过应用 2.6 的低截断评分,可准确排除 PVT 事件(阴性预测值 94%)。使用 4.6 的高截断评分(阳性预测值 85%),可高度准确地诊断 PVT。PVT-RI 可预测等待救命性肝移植的候选者是否会发生未来的 PVT。尽管该评分系统需要前瞻性验证,但它为临床医生在肝移植前对肝硬化患者进行风险分层以预测未来 PVT 发展提供了一种强大的新工具。