Department of Nephrology, Fujita Health University School of Medicine, Toyoake, Japan.
The Aichi Cohort Study of Prognosis in Patients Newly Initiated into Dialysis (AICOPP) Group, Aichi, Japan.
PLoS One. 2019 Aug 22;14(8):e0221352. doi: 10.1371/journal.pone.0221352. eCollection 2019.
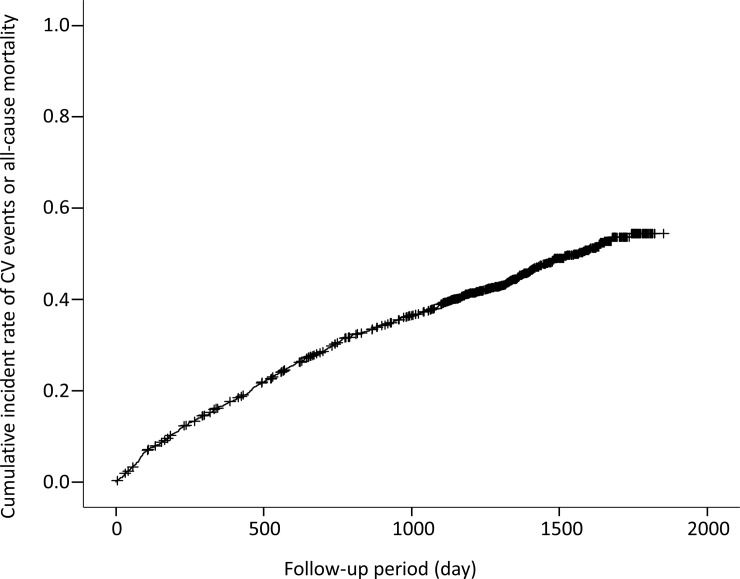
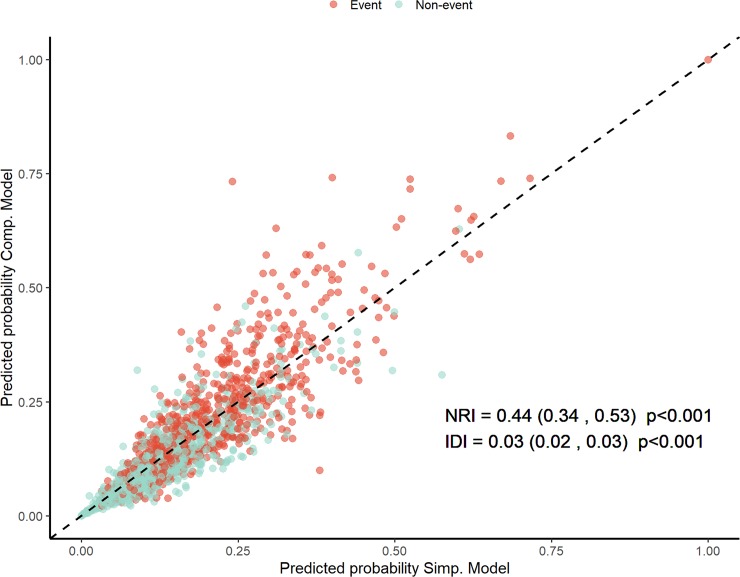
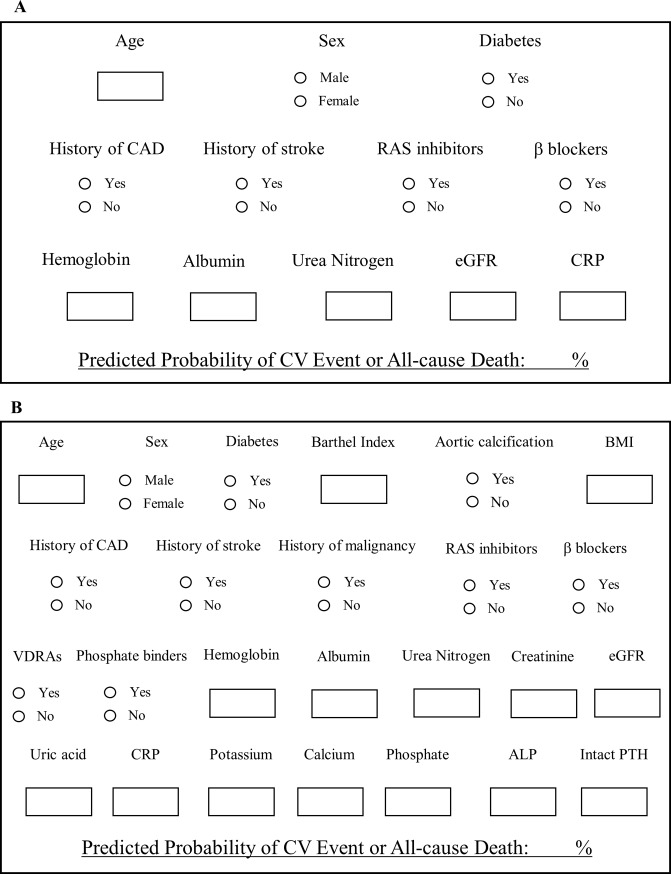
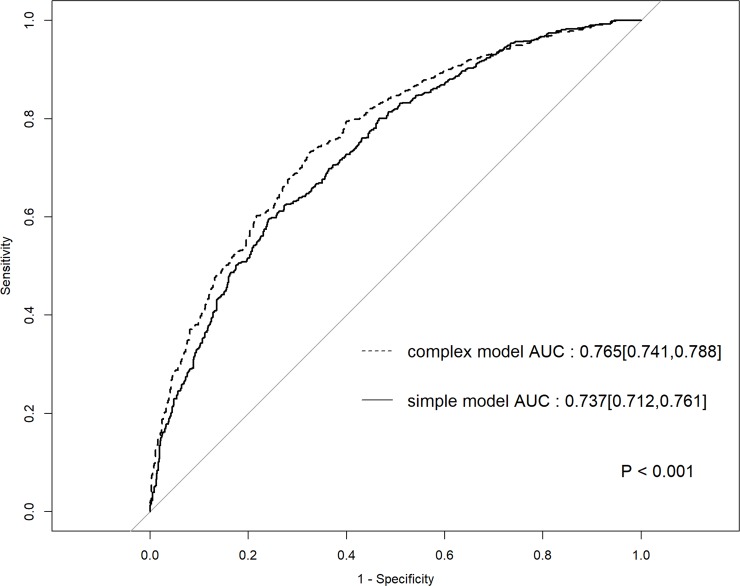
Some variables including age, comorbidity of diabetes, and so on at dialysis initiation are associated with patient prognosis. Cardiovascular (CV) events are a major cause of death, and adequate models that predict prognosis in dialysis patients are warranted. Therefore, we created models using some variables at dialysis initiation. We used a database of 1,520 consecutive dialysis patients (median age, 70 years; 492 women [32.4%]) from a multicenter prospective cohort study. We established the primary endpoint as a composite of the incidence of first CV events or all-cause death. A multivariable Cox proportional hazard regression model was used to construct a model. We considered a complex and a simple model. We used area under the receiver operating characteristic curve (AUROC) to assess and compare the predictive performances of the prediction models and evaluated the improvement in discrimination using the complex model versus the simple model using net reclassification improvement (NRI). We then assessed integrated discrimination improvement (IDI) to evaluate improvements in average sensitivity and specificity. Of 392 deaths, 152 were CV-related. Totally, 506 CV events occurred during the follow-up period (median 1,285 days). Finally, 692 patients reached the primary endpoint. Baseline data were set at dialysis initiation. AUROC for the primary endpoint was 0.737 (95% confidence interval [CI], 0.712-0.761) in the simple model and 0.765 (95% CI, 0.741-0.788) in the complex model. There were significant intergroup differences in NRI (0.44; 95% CI, 0.34-0.53; p < 0.001) and IDI (0.02; 95% CI, 0.02-0.03; p < 0.001). We prepared a Shiny R application for each model to automatically calculate the predicted occurrence probability (https://statacademy.shinyapps.io/App_inaguma_20190717/). The complex model made more accurate predictions than the simple model. However, the intergroup difference was not significant. Hence, the simple model was more useful than the complex model. The tool was useful in a real-world clinical setting because it required only routinely available variables. Moreover, we emphasized that the tool could predict the incidence of CV events or all-cause mortality for individual patients. In the future, we must confirm its external validity in other prospective cohorts.
一些变量,包括透析开始时的年龄、糖尿病合并症等,与患者预后相关。心血管(CV)事件是死亡的主要原因,需要有足够的模型来预测透析患者的预后。因此,我们使用透析开始时的一些变量建立了模型。我们使用了一项来自多中心前瞻性队列研究的 1520 例连续透析患者(中位年龄 70 岁;492 名女性[32.4%])的数据库。我们将主要终点定义为首次 CV 事件或全因死亡的复合终点。使用多变量 Cox 比例风险回归模型构建模型。我们考虑了复杂模型和简单模型。我们使用接收者操作特征曲线下面积(AUROC)来评估和比较预测模型的预测性能,并使用净重新分类改善(NRI)来评估复杂模型与简单模型相比在区分度上的改善。然后,我们评估综合判别改善(IDI)以评估平均敏感性和特异性的改善。在 392 例死亡中,有 152 例与 CV 相关。在随访期间共发生 506 例 CV 事件(中位随访时间为 1285 天)。最后,有 692 例患者达到了主要终点。基线数据设定在透析开始时。简单模型中主要终点的 AUROC 为 0.737(95%置信区间[CI],0.712-0.761),复杂模型中为 0.765(95%CI,0.741-0.788)。NRI(0.44;95%CI,0.34-0.53;p<0.001)和 IDI(0.02;95%CI,0.02-0.03;p<0.001)存在显著的组间差异。我们为每个模型准备了一个 Shiny R 应用程序,用于自动计算预测发生概率(https://statacademy.shinyapps.io/App_inaguma_20190717/)。复杂模型的预测比简单模型更准确。然而,两组间的差异并不显著。因此,简单模型比复杂模型更有用。该工具在实际临床环境中非常有用,因为它只需要常规可用的变量。此外,我们强调该工具可以预测个体患者的 CV 事件或全因死亡率。未来,我们必须在其他前瞻性队列中确认其外部有效性。