Pong Jeremy Zhenwen, Koh Zhi Xiong, Samsudin Mas'uud Ibnu, Fook-Chong Stephanie, Liu Nan, Ong Marcus Eng Hock
Duke-NUS Medical School, National University of Singapore.
Department of Emergency Medicine, Singapore General Hospital.
Medicine (Baltimore). 2019 Aug;98(34):e16962. doi: 10.1097/MD.0000000000016962.
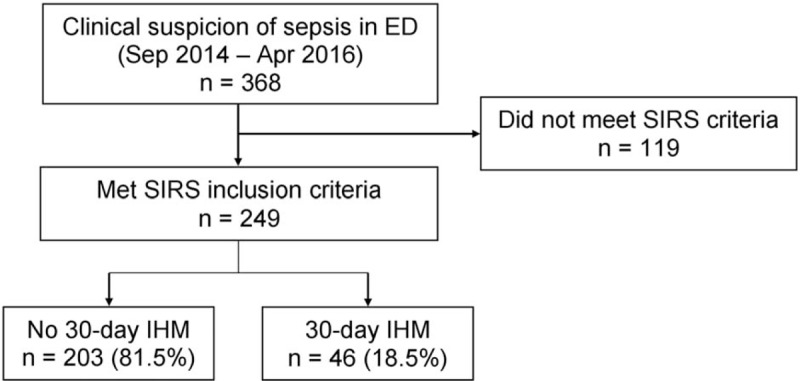
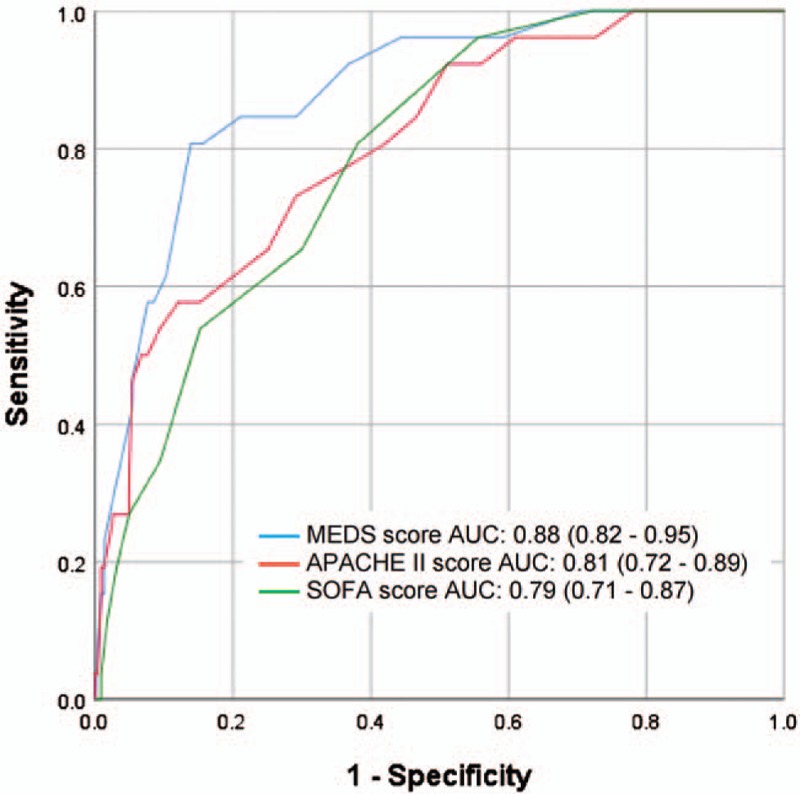
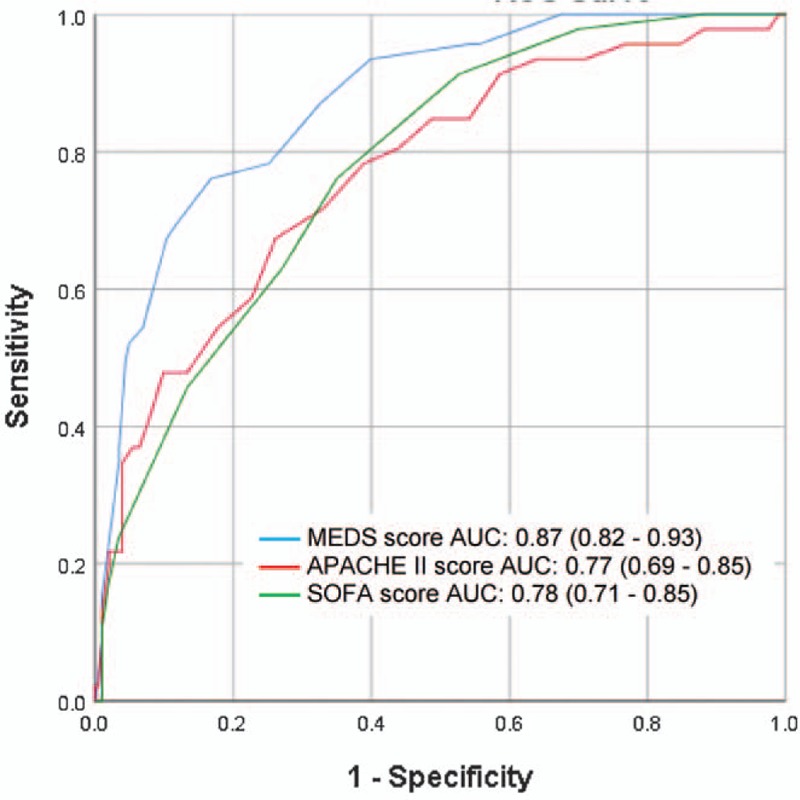
The emergency department (ED) serves as the first point of hospital contact for most septic patients. Early mortality risk stratification using a quick and accurate triage tool would have great value in guiding management. The mortality in emergency department sepsis (MEDS) score was developed to risk stratify patients presenting to the ED with suspected sepsis, and its performance in the literature has been promising. We report in this study the first utilization of the MEDS score in a Singaporean cohort.In this retrospective observational cohort study, adult patients presenting to the ED with suspected sepsis and fulfilling systemic inflammatory response syndrome (SIRS) criteria were recruited. Primary outcome was 30-day in-hospital mortality (IHM) and secondary outcome was 72-hour mortality. MEDS, acute physiology and chronic health evaluation II (APACHE II), and sequential organ failure assessment (SOFA) scores were compared for prediction of primary and secondary outcomes. Receiver operating characteristic (ROC) analysis was conducted to compare predictive performance.Of the 249 patients included in the study, 46 patients (18.5%) met 30-day IHM. MEDS score achieved an area under the ROC curve (AUC) of 0.87 (95% confidence interval [CI], 0.82-0.93), outperforming the APACHE II score (0.77, 95% CI 0.69-0.85) and SOFA score (0.78, 95% CI 0.71-0.85). On secondary analysis, MEDS score was superior to both APACHE II and SOFA scores in predicting 72-hour mortality, with AUC of 0.88 (95% CI 0.82-0.95), 0.81 (95% CI 0.72-0.89), and 0.79 (95% CI 0.71-0.87), respectively. In predicting 30-day IHM, MEDS score ≥12, APACHE II score ≥23, and SOFA score ≥5 performed at sensitivities of 76.1%, 67.4%, and 76.1%, and specificities of 83.3%, 73.9%, and 65.0%, respectively.The MEDS score performed well in its ability for mortality risk stratification in a Singaporean ED cohort.
急诊科(ED)是大多数脓毒症患者与医院接触的第一站。使用快速准确的分诊工具进行早期死亡风险分层对指导治疗具有重要价值。急诊科脓毒症(MEDS)评分旨在对疑似脓毒症的急诊科患者进行死亡风险分层,其在文献中的表现很有前景。我们在本研究中报告了MEDS评分在新加坡队列中的首次应用。
在这项回顾性观察队列研究中,招募了因疑似脓毒症就诊于急诊科且符合全身炎症反应综合征(SIRS)标准的成年患者。主要结局是30天院内死亡率(IHM),次要结局是72小时死亡率。比较MEDS、急性生理与慢性健康状况评估II(APACHE II)和序贯器官衰竭评估(SOFA)评分对主要和次要结局的预测能力。进行受试者操作特征(ROC)分析以比较预测性能。
在纳入研究的249例患者中,46例(18.5%)达到30天IHM。MEDS评分的ROC曲线下面积(AUC)为0.87(95%置信区间[CI],0.82 - 0.93),优于APACHE II评分(0.77,95% CI 0.69 - 0.85)和SOFA评分(0.78,95% CI 0.71 - 0.85)。在二次分析中,MEDS评分在预测72小时死亡率方面优于APACHE II和SOFA评分,AUC分别为0.88(95% CI 0.82 - 0.95)、0.81(95% CI 0.72 - 0.89)和0.79(95% CI 0.71 - 0.87)。在预测30天IHM时,MEDS评分≥12、APACHE II评分≥23和SOFA评分≥5的敏感性分别为76.1%、67.4%和76.1%,特异性分别为83.3%、73.9%和65.0%。
MEDS评分在新加坡急诊科队列的死亡风险分层能力方面表现良好。