Department of Medicine, Endocrine Unit, Massachusetts General Hospital, Havard Medical School, Boston, MA, USA.
Biostatistics Center, Massachusetts General Hospital, Havard Medical School, Boston, MA, USA.
Lancet Diabetes Endocrinol. 2019 Oct;7(10):767-775. doi: 10.1016/S2213-8587(19)30255-4. Epub 2019 Aug 22.
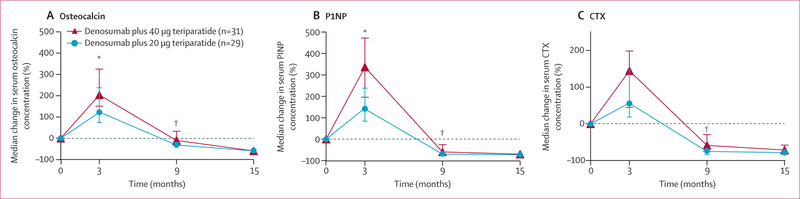
In the Denosumab and Teriparatide Administration (DATA) study, we showed that denosumab fully inhibits teriparatide-induced bone resorption while allowing for continued teriparatide-induced bone formation, resulting in larger increases in hip and spine bone mineral density (BMD) than with either drug alone. We aimed to assess whether administration of denosumab with high dose teriparatide would stimulate larger increases in bone mass than those observed in the DATA study.
DATA-HD was an open-label, randomised, controlled phase 4 trial done at Massachusetts General Hospital. Eligible women were postmenopausal women (at least 36 months since last menses or since hysterectomy with a follicle-stimulating hormone concentration of ≥40 U/L) with osteoporosis. Participants were randomly assigned (1:1) to receive teriparatide 20 μg (standard dose) or 40 μg (high dose) daily via subcutaneous injection for 9 months. At 3 months, both groups were started on denosumab 60 mg every 6 months via subcutaneous injection for 12 months. Areal BMD (aBMD) was measured at 0, 3, 9, and 15 months. Treatment was given open label, but outcome assessors were masked. The primary endpoint was percentage change from baseline in spine areal BMD (aBMD) at 15 months. Women who completed at least one study visit after baseline were included in the modified intention-to-treat analysis. Safety was assessed in all randomly assigned participants. This study is registered with ClinicalTrials.gov, number NCT02176382.
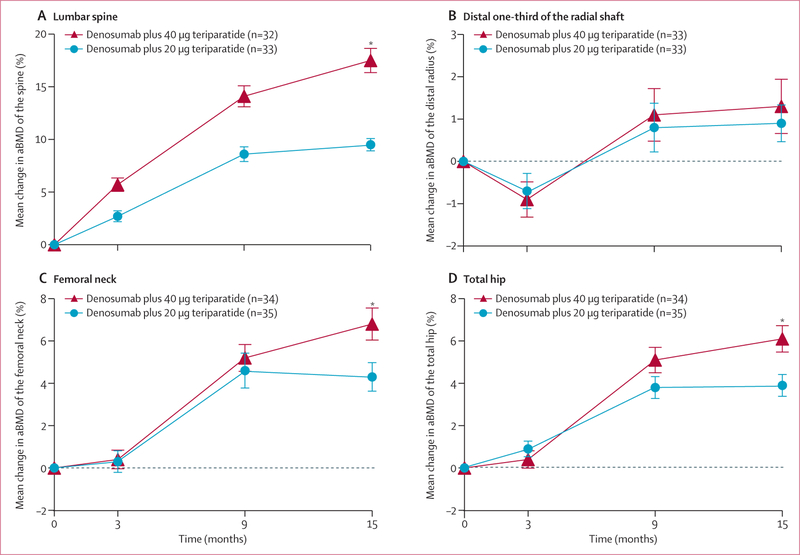
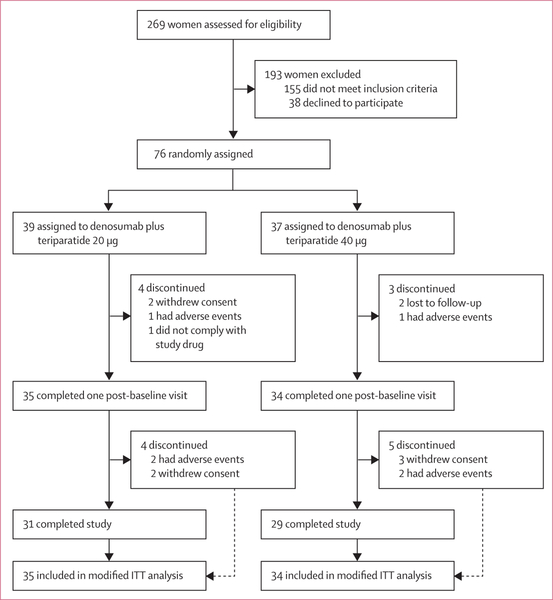
Between Oct 15, 2014, and June 10, 2016, 269 women were assessed for eligibility. 76 participants were randomly assigned to 20 μg teriparatide (n=39) or 40 μg teriparatide (n=37), of whom 69 completed at least one post-baseline visit. At 15 months, mean spine aBMD had increased to a significantly greater extent in the 40 μg group (17·5% [SD 6·0] increase) than the 20 μg group (9·5% [3·2]; difference 8·1%, 95% CI 5·5 to 10·6, p<0·0001). Mean femoral neck aBMD had also increased to a greater extent in the 40 μg group (6·8% [SD 4·1] increase) than the 20 μg group (4·3% [3·7]; difference 2·5%, 0·5 to 4·5, p=0·04), as did mean total hip aBMD (40 μg group, 6·1% [3·4] increase; 20 μg group, 3·9% [2·9] increase; difference 2·2%, 0·6 to 3·8, p<0·0001). 30 (77%) of 39 participants in the 20 μg group and 29 (78%) of 37 participants in the 40 μg group had an adverse event, and seven (18%) and two (5%) patients had serious adverse events. The most frequent adverse events were joint pain (15 [38%]), muscle cramp (15 [38%]), and fatigue (12 [31%]) in the 20 μg group group and fatigue (14 [38%]), nausea (16 [43%]), and joint pain (17 [46%]) in the 40 μg group. No deaths were reported.
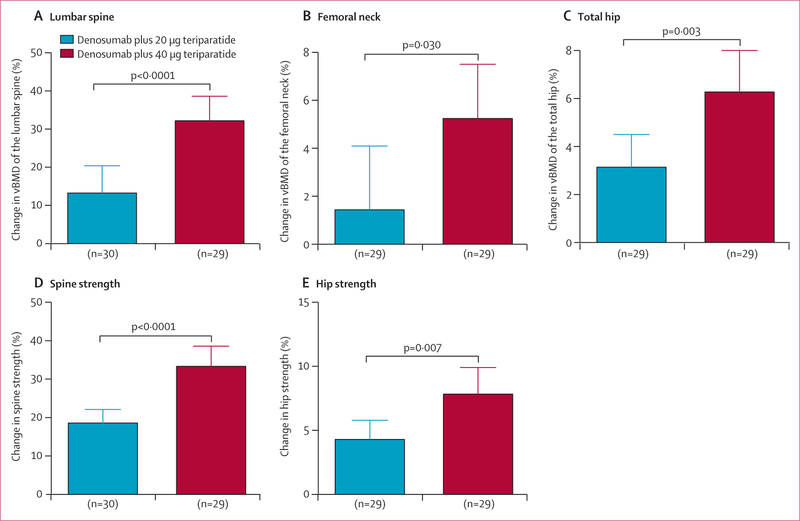
Combined treatment with teriparatide 40 μg and denosumab increases spine and hip BMD more than standard combination therapy. This large and rapid increase in bone mass suggest that this high dose regimen might provide a method of restoring skeletal integrity in patients with osteoporosis.
National Institutes of Health and the Dart Foundation.
在 Denosumab 和 Teriparatide 给药(DATA)研究中,我们表明 denosumab 完全抑制了 teriparatide 引起的骨吸收,同时允许继续进行 teriparatide 引起的骨形成,从而导致髋部和脊柱骨密度(BMD)的增加大于单独使用任何一种药物。我们旨在评估 denosumab 联合高剂量 teriparatide 是否会刺激比 DATA 研究中观察到的更大的骨量增加。
DATA-HD 是一项在马萨诸塞州综合医院进行的开放性、随机、对照的 4 期临床试验。符合条件的女性为绝经后妇女(至少 36 个月绝经或子宫切除后卵泡刺激素浓度≥40 U/L)伴骨质疏松症。参与者被随机分配(1:1)接受每日皮下注射 20 μg(标准剂量)或 40 μg(高剂量)的 teriparatide 9 个月。在 3 个月时,两组均开始每 6 个月皮下注射 60 mg denosumab 12 个月。在 0、3、9 和 15 个月时测量面积骨密度(aBMD)。治疗是开放标签的,但结果评估者是盲法的。主要终点是 15 个月时脊柱面积骨密度(aBMD)与基线相比的百分比变化。至少完成一次基线后研究访问的女性被纳入改良意向治疗分析。所有随机分配的参与者均进行了安全性评估。该研究在 ClinicalTrials.gov 注册,编号为 NCT02176382。
在 2014 年 10 月 15 日至 2016 年 6 月 10 日期间,有 269 名女性接受了入选评估。76 名参与者被随机分配到 20 μg teriparatide 组(n=39)或 40 μg teriparatide 组(n=37),其中 69 名完成了至少一次基线后访问。在 15 个月时,40 μg 组的脊柱 aBMD 增加到显著更大的程度(17.5%[6.0]增加),而 20 μg 组为 9.5%[3.2];差异为 8.1%,95%CI 5.5 至 10.6,p<0.0001)。40 μg 组的股骨颈 aBMD 也增加到更大的程度(6.8%[4.1]增加),而 20 μg 组为 4.3%[3.7];差异为 2.5%,0.5 至 4.5,p=0.04),总髋关节 aBMD 也增加到更大的程度(40 μg 组,6.1%[3.4]增加;20 μg 组,3.9%[2.9]增加;差异 2.2%,0.6 至 3.8,p<0.0001)。20 μg 组 39 名参与者中的 30 名(77%)和 40 μg 组 37 名参与者中的 29 名(78%)发生了不良事件,7 名(18%)和 2 名(5%)患者发生了严重不良事件。最常见的不良事件是关节痛(15[38%])、肌肉痉挛(15[38%])和疲劳(12[31%])在 20 μg 组,而疲劳(14[38%])、恶心(16[43%])和关节痛(17[46%])在 40 μg 组。没有报告死亡。
联合使用 teriparatide 40 μg 和 denosumab 可增加脊柱和髋关节 BMD 大于标准联合治疗。这种骨量的大量快速增加表明,这种高剂量方案可能为骨质疏松症患者提供恢复骨骼完整性的方法。
美国国立卫生研究院和 Dart 基金会。