Hughes Ryan T, Helis Corbin A, Soike Michael H, Levine Beverly J, Farris Michael, Blackstock Arthur W
Radiation Oncology, Wake Forest School of Medicine, Winston-Salem, USA.
Epidemiology, Wake Forest School of Medicine, Winston-Salem, USA.
Cureus. 2019 Jun 22;11(6):e4969. doi: 10.7759/cureus.4969.
The optimal management of patients with early non-small cell lung cancer (NSCLC) not amenable to surgical resection or stereotactic body radiotherapy (SBRT) or those with hilar nodal involvement ineligible for surgery or concurrent chemoradiotherapy is unclear. This report describes survival outcomes and toxicity profiles of patients treated with hypofractionated radiotherapy (HRT) alone.
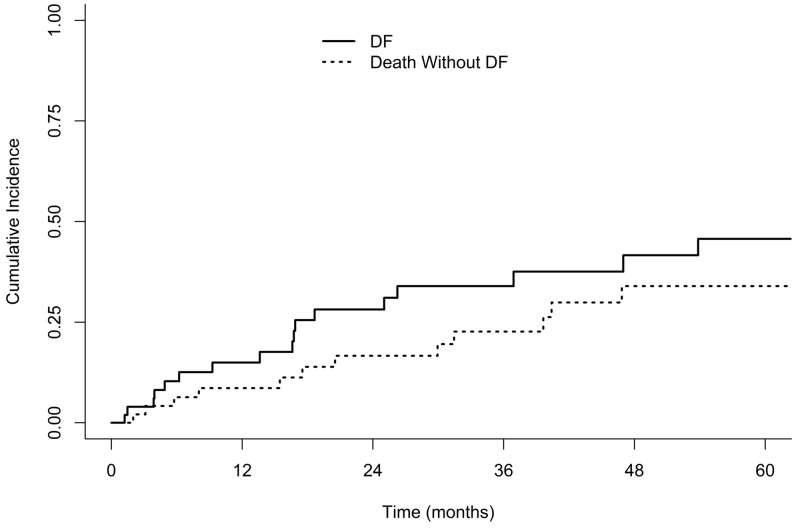
A total of 52 patients with Stage I-IIB NSCLC treated with HRT alone between 2010-2018 were reviewed. Patients were categorized as having ultracentral tumors if the planning target volume contacted or overlapped the proximal bronchial tree, esophagus, pulmonary vein or artery. Overall survival (OS) and progression-free survival (PFS) were estimated using the Kaplan-Meier method and the competing risk cumulative incidence of locoregional failure (LRF) and distant failure (DF) were estimated using death without failure as a competing risk. Pneumonitis and esophagitis rates were evaluated as per Acute Common Terminology Criteria for Adverse Events (CTCAE) version 4.0.
Of the 52 patients analyzed, 50 patients were treated with radiotherapy alone to a dose of 70.2 Gy in 26 fractions, one patient was treated with 68 Gy in 25 fractions and one patient was treated with 65 Gy in 26 fractions. The median age was 72 (range 48-89), 42% of patients had an Eastern Cooperative Oncology Group (ECOG) performance status of 2-3, 46% were stage I and 54% were stage II. Hilar nodal involvement was present in 21% of patients and 74% of node-negative patients had ultracentral primary tumors. Median OS was 39.6 months and the median PFS was 21.0 months. Overall three-year cumulative incidence of LRF and DF were 32% and 34%, respectively. Grade 3 pneumonitis occurred in two (4%) patients. No grade 3+ acute esophagitis or grade 4-5 toxicities were observed.
Hypofractionated thoracic radiotherapy consisting of 70.2 Gy is well-tolerated and results in favorable locoregional control for stage I-IIB patients who are not candidates for SBRT, surgery, or concurrent chemoradiotherapy.
对于无法进行手术切除或立体定向体部放疗(SBRT)的早期非小细胞肺癌(NSCLC)患者,或那些肺门淋巴结受累而不适合手术或同步放化疗的患者,最佳治疗方案尚不清楚。本报告描述了单纯接受大分割放疗(HRT)患者的生存结果和毒性特征。
回顾了2010年至2018年间共52例仅接受HRT治疗的I-IIB期NSCLC患者。如果计划靶体积接触或重叠近端支气管树、食管、肺静脉或动脉,则将患者分类为具有超中央肿瘤。采用Kaplan-Meier方法估计总生存期(OS)和无进展生存期(PFS),并以无失败死亡作为竞争风险估计局部区域失败(LRF)和远处失败(DF)的竞争风险累积发生率。根据急性不良事件通用术语标准(CTCAE)第4.0版评估肺炎和食管炎发生率。
在分析的52例患者中,50例患者仅接受放疗,剂量为70.2 Gy,分26次;1例患者接受68 Gy,分25次;1例患者接受65 Gy,分26次。中位年龄为72岁(范围48-89岁),42%的患者东部肿瘤协作组(ECOG)体能状态为2-3,46%为I期,54%为II期。21%的患者存在肺门淋巴结受累,74%的淋巴结阴性患者有超中央原发性肿瘤。中位OS为39.6个月,中位PFS为21.0个月。LRF和DF的总体三年累积发生率分别为32%和34%。2例(4%)患者发生3级肺炎。未观察到3级以上急性食管炎或4-5级毒性反应。
对于不适合SBRT、手术或同步放化疗的I-IIB期患者,70.2 Gy的大分割胸部放疗耐受性良好,并能实现良好的局部区域控制。