Department of Respiratory Critical Care Medicine, The First Affiliated Hospital of Guangxi Medical University, Nanning, 530021, Guangxi, China.
BMC Infect Dis. 2019 Aug 27;19(1):745. doi: 10.1186/s12879-019-4376-6.
Due to the similar clinical, lung imaging, and pathological characteristics, talaromycosis is most commonly misdiagnosed as tuberculosis. This study aimed to identify the characteristics of talaromycosis pleural effusion (TMPE) and to distinguish TMPE from tuberculosis pleural effusion (TPE).
We enrolled 19 cases each of TMPE and TPE from Guangxi, China. Patients' clinical records, pleural effusion tests, biomarker test results, and receiver operating characteristic curves were analyzed.
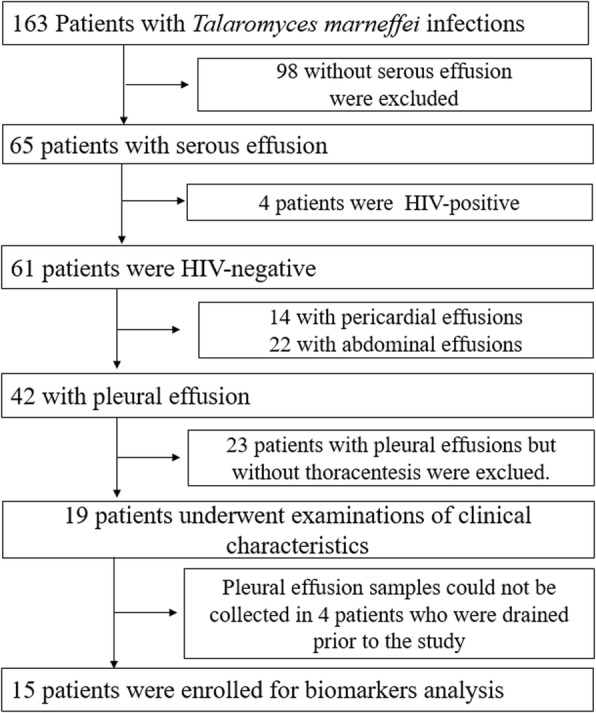
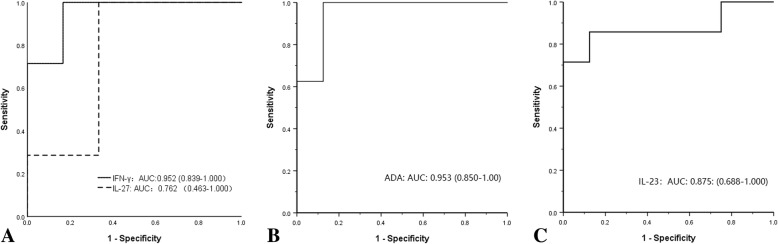
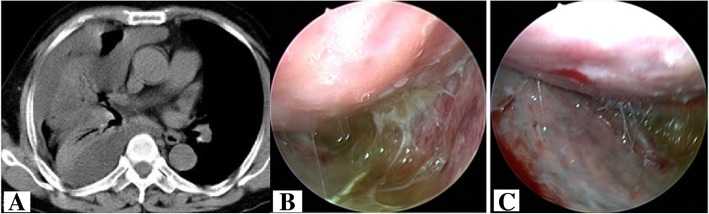
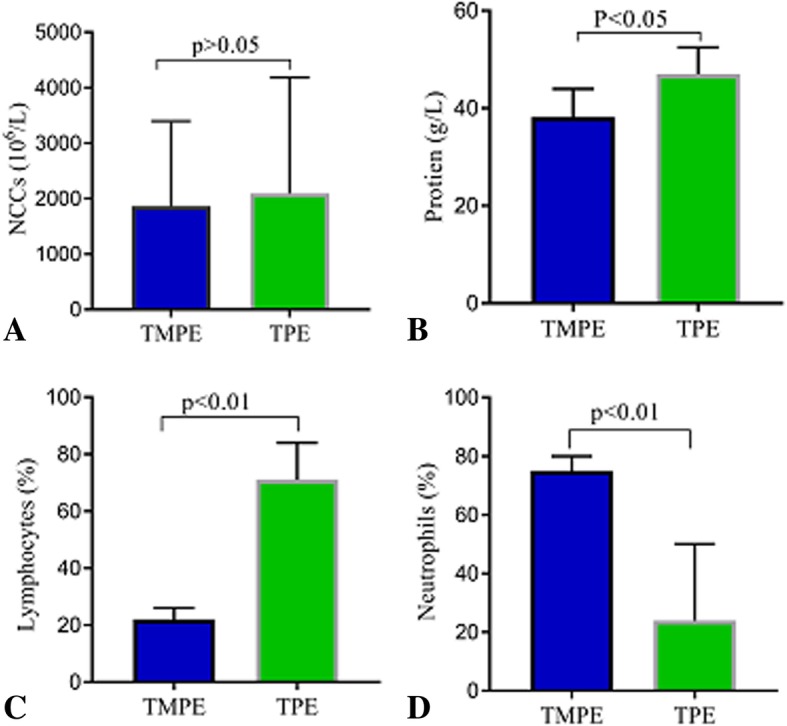
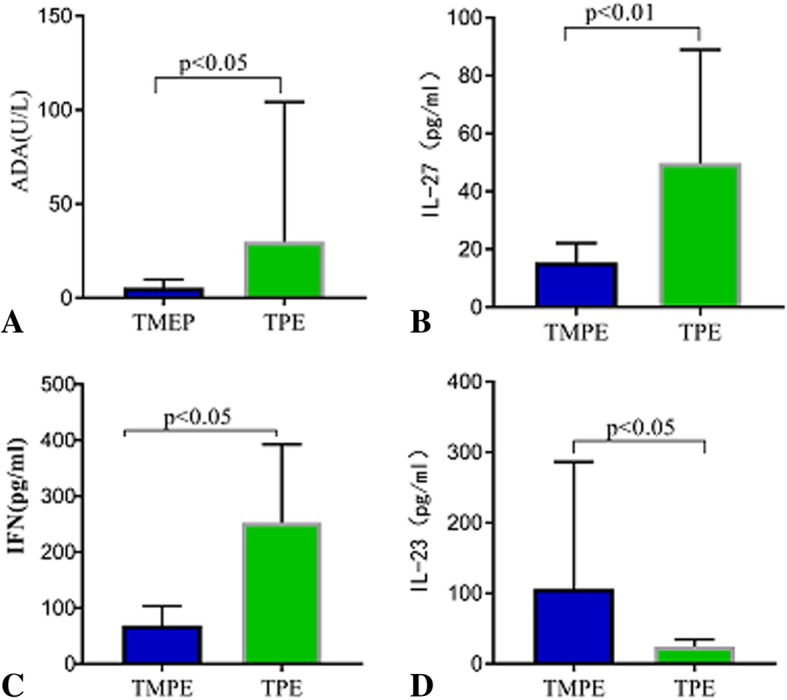
In total, 39.8% (65/163) of patients exhibited serous effusion, of whom 61 were non-human immunodeficiency virus (HIV)-infected patients; 68.85% of the non-HIV-infected patients (42/61) had TMPE. Thoracentesis was performed only in 19 patients, all of whom were misdiagnosed with tuberculosis and received long-term anti-tuberculosis treatment. In four of these patients, interleukin (IL)-23, IL-27, and interferon-gamma (IFN-γ) measurements were not performed since pleural effusion samples could not be collected because the effusion had been drained prior to the study. In the remaining 15 patients, pleural effusion samples were collected. Talaromyces marneffei was isolated from the pleural effusion and pleural nodules. Most TMPEs were characterized by yellowish fluid, with marked elevation of protein content and nucleated cell counts. However, neutrophils were predominantly found in TMPEs, and lymphocytes were predominantly found in TPEs (both p < 0.05). Adenosine deaminase (ADA) and IFN-γ levels in TMPEs were significantly lower than those in TPEs (all p < 0.05) and provided similar accuracies for distinguishing TMPEs from TPEs. IL-23 concentration in TMPEs was significantly higher than that in TPEs (p < 0.05), and it provided similar accuracy for diagnosing TMPEs. IL-27 concentrations in TMPEs were significantly lower than those in TPEs (all p < 0.05) but was not useful for distinguishing TMPE from TPE.
Talaromycosis can infringe on the pleural cavity via the translocation of T. marneffei into the pleural space. Nonetheless, this phenomenon is still commonly neglected by clinicians. TMPE is a yellowish fluid with exudative PEs and predominant neutrophils. Higher neutrophil counts and IL-23 may suggest talaromycosis. Higher lymphocyte counts, ADA activity, and IFN-γ concentration may suggest tuberculosis.
由于临床表现、肺部影像学和病理学特征相似,马尔尼菲青霉病常被误诊为结核病。本研究旨在确定马尔尼菲青霉性胸腔积液(TMPE)的特征,并将其与结核性胸腔积液(TPE)区分开来。
我们从中国广西招募了 19 例 TMPE 和 19 例 TPE 患者。分析了患者的临床记录、胸腔积液检查、生物标志物检测结果和受试者工作特征曲线。
共有 39.8%(65/163)的患者表现为浆液性胸腔积液,其中 61 例患者未感染人类免疫缺陷病毒(HIV);61 例非 HIV 感染患者中有 68.85%(42/61)为 TMPE。仅对 19 例患者进行了胸腔穿刺,所有患者均被误诊为结核病,并接受了长期抗结核治疗。其中 4 例由于在研究前已引流胸腔积液,无法采集胸腔积液样本,因此未进行白细胞介素(IL)-23、IL-27 和干扰素-γ(IFN-γ)检测。其余 15 例患者采集了胸腔积液样本。从胸腔积液和胸腔结节中分离出马尔尼菲青霉。大多数 TMPE 的特征是黄色液体,蛋白含量和有核细胞计数明显升高。然而,TMPE 中主要发现中性粒细胞,TPE 中主要发现淋巴细胞(均 p<0.05)。TMPE 中的腺苷脱氨酶(ADA)和 IFN-γ水平明显低于 TPE(均 p<0.05),并能以相似的准确度区分 TMPE 和 TPE。TMPE 中的 IL-23 浓度明显高于 TPE(p<0.05),对诊断 TMPE 也具有相似的准确性。TMPE 中的 IL-27 浓度明显低于 TPE(均 p<0.05),但对区分 TMPE 和 TPE 没有帮助。
马尔尼菲青霉可通过 T. marneffei 转移至胸膜腔侵犯胸膜腔。尽管如此,临床医生仍常忽略这种现象。TMPE 是一种黄色液体,渗出性胸腔积液,以中性粒细胞为主。较高的中性粒细胞计数和 IL-23 可能提示马尔尼菲青霉病。较高的淋巴细胞计数、ADA 活性和 IFN-γ 浓度可能提示结核病。