National Clinical Laboratory on Tuberculosis, Beijing Key Laboratory for Drug Resistant Tuberculosis Research, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis and Thoracic Tumor Institute, Beijing, China.
Department of Tuberculosis, Beijing Chest Hospital, Capital Medical University, Beijing Tuberculosis and Thoracic Tumor Institute, Beiguan St #9, Beijing, 101149, China.
BMC Infect Dis. 2021 Jan 4;21(1):4. doi: 10.1186/s12879-020-05676-2.
Tuberculous pleural effusion (TPE) is the most common extrapulmonary manifestation and may have lasting effect on lung function. However conventional diagnostic tests for TPE register multiple limitations. This study estimates diagnostic efficacy of the interferon gamma release assay (IGRA: T-SPOT.TB) in TPE patients of different characteristics.
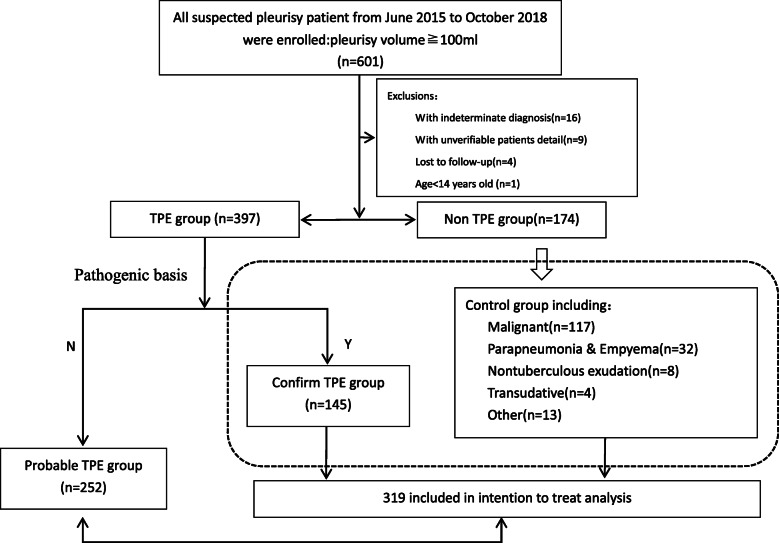
We performed a prospective, single-centre study including all suspected pleural effusion patients consecutively enrolled from June 2015 to October 2018. Through receiver operating characteristic (ROC) curves, technical cut-offs and the utility of T-SPOT on pleural fluid (PF) were determined and analysed. Logistic regression analysis was performed to obtain the independent risk factors for TPE, and evaluated the performance of the T-SPOT assay stratified by risk factors in comparison to ADA.
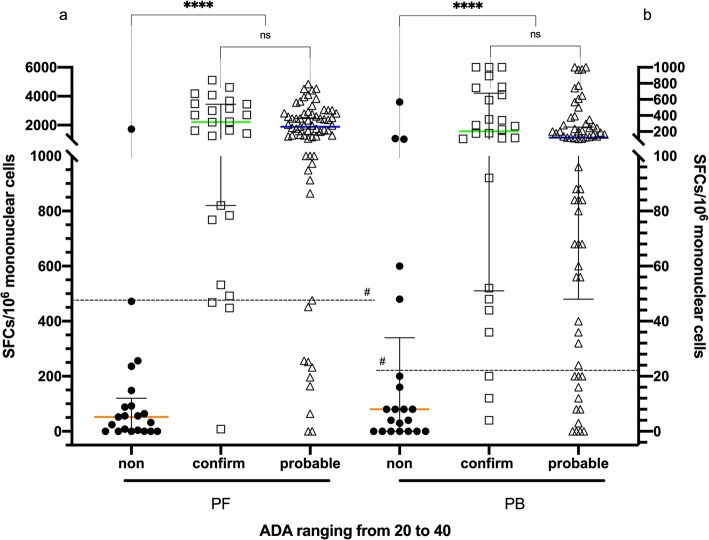
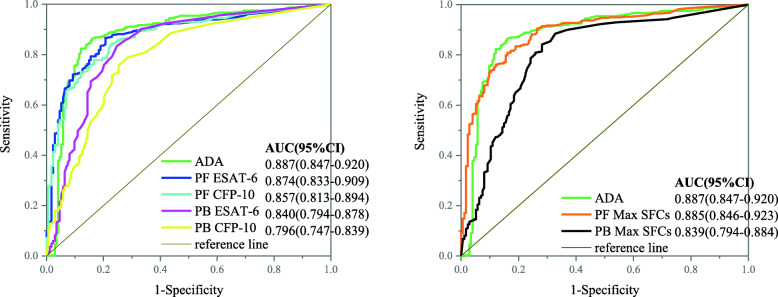
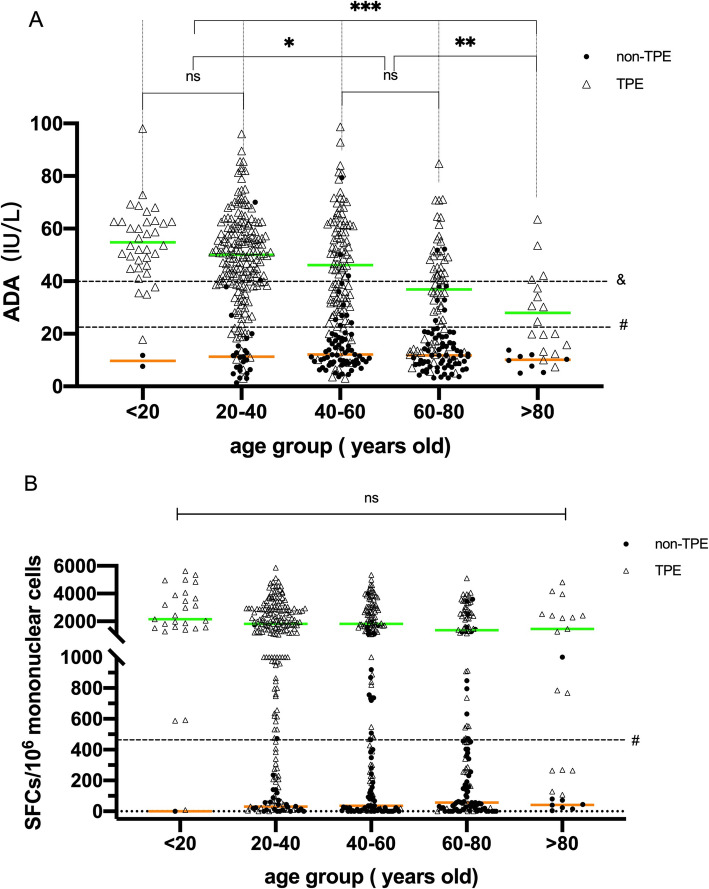
A total of 601 individuals were consecutively recruited. The maximum spot-forming cells (SFCs) of early secretory antigenic target-6 (ESAT-6) and culture filtrate protein-10 (CFP-10) in the PF T-SPOT assay had the best diagnostic efficiency in our study, which was equal to ADA (0.885 vs 0.887, P = 0.957) and superior to peripheral blood (PB), with a sensitivity of 83.0% and a specificity of 83.1% (The cut-off value was 466 SFCs/10 mononuclear cells). Among the TPE patients with low ADA (< 40 IU/L), the sensitivity and specificity of PF T-SPOT were still 87.9 and 90.5%, respectively. The utility of ADA was negatively related to increasing age, but the PF T-SPOT test had a steady performance at all ages. Age (< 45 yrs.; odds ratio (OR) = 5.61, 95% confidence interval (CI) 3.59-8.78; P < 0.001), gender (male; OR = 2.68, 95% CI 1.75-2.88; P < 0.001) and body mass index (BMI) (< 22; OR = 1.93, 95% CI 1.30-2.88; P = 0.001) were independently associated with the risk of TB by multivariate logistic regression analysis. Notably, when stratified by risk factor, the sensitivity of PF T-SPOT was superior to the sensitivity for ADA (76.5% vs. 23.5%, P = 0.016) and had noninferior specificity (84.4% vs. 96.9%, P = 0.370).
In conclusion, the PF T-SPOT assay can effectively discriminate TPE patients whose ADA is lower than 40 IU/L and is superior to ADA in unconventional TPE patients (age ≥ 45 yrs., female or BMI ≥ 22). The PF T-SPOT assay is an excellent choice to supplement ADA to diagnose TPE.
结核性胸腔积液(TPE)是最常见的肺外表现,可能对肺功能产生持久影响。然而,传统的 TPE 诊断测试存在多种局限性。本研究旨在评估干扰素γ释放试验(IGRA:T-SPOT.TB)在不同特征的 TPE 患者中的诊断效能。
我们进行了一项前瞻性、单中心研究,纳入了 2015 年 6 月至 2018 年 10 月连续入组的所有疑似胸腔积液患者。通过受试者工作特征(ROC)曲线、技术截断值和 T-SPOT 在胸腔积液(PF)中的应用,确定并分析了 T-SPOT 的诊断效能。通过多因素 logistic 回归分析获得 TPE 的独立危险因素,并评估了 T-SPOT 试验在危险因素分层下与 ADA 相比的性能。
共纳入 601 例患者。PF T-SPOT 试验中早期分泌抗原靶-6(ESAT-6)和培养滤液蛋白-10(CFP-10)的最大斑点形成细胞(SFC)具有最佳的诊断效率,与 ADA(0.885 比 0.887,P=0.957)相当,优于外周血(PB),其灵敏度为 83.0%,特异性为 83.1%(截断值为 466 SFC/10 个单核细胞)。在 ADA 较低(<40IU/L)的 TPE 患者中,PF T-SPOT 的灵敏度和特异性仍分别为 87.9%和 90.5%。ADA 的效能与年龄的增加呈负相关,但 PF T-SPOT 试验在所有年龄段的性能均较稳定。年龄(<45 岁;比值比(OR)=5.61,95%置信区间(CI)3.59-8.78;P<0.001)、性别(男性;OR=2.68,95%CI 1.75-2.88;P<0.001)和体重指数(BMI)(<22;OR=1.93,95%CI 1.30-2.88;P=0.001)是多因素 logistic 回归分析中与 TB 风险相关的独立危险因素。值得注意的是,当按危险因素分层时,PF T-SPOT 的灵敏度优于 ADA(76.5%比 23.5%,P=0.016),特异性相当(84.4%比 96.9%,P=0.370)。
总之,PF T-SPOT 试验可有效鉴别 ADA 低于 40IU/L 的 TPE 患者,且在非典型 TPE 患者(年龄≥45 岁、女性或 BMI≥22)中优于 ADA。PF T-SPOT 试验是补充 ADA 诊断 TPE 的优秀选择。