Janssen Research & Development, LLC, Titusville, New Jersey.
Janssen Research & Development, LLC, Raritan, New Jersey.
Pharmacoepidemiol Drug Saf. 2019 Dec;28(12):1620-1628. doi: 10.1002/pds.4887. Epub 2019 Aug 27.
To compare the incidence of diabetic ketoacidosis (DKA) among patients with type 2 diabetes mellitus (T2DM) who were new users of sodium glucose co-transporter 2 inhibitors (SGLT2i) versus other classes of antihyperglycemic agents (AHAs).
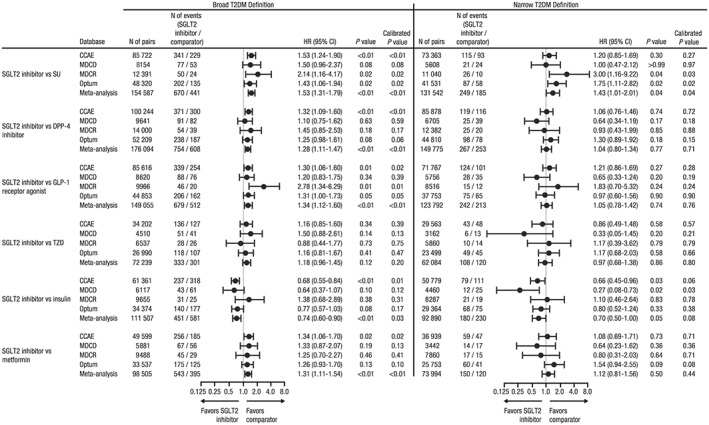
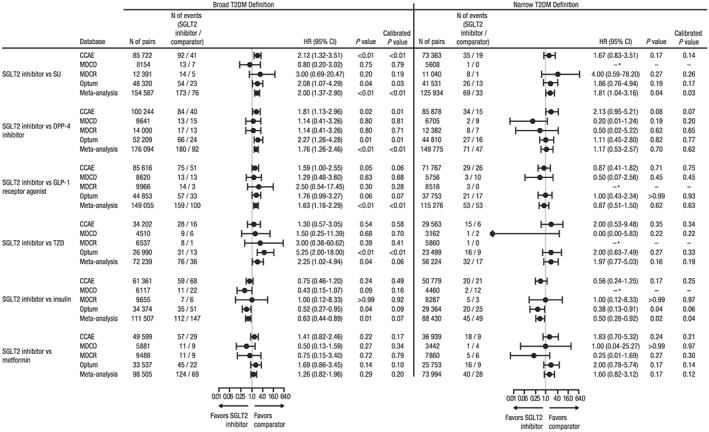
Patients were identified from four large US claims databases using broad (all T2DM patients) and narrow (intended to exclude patients with type 1 diabetes or secondary diabetes misclassified as T2DM) definitions of T2DM. New users of SGLT2i and seven groups of comparator AHAs were matched (1:1) on exposure propensity scores to adjust for imbalances in baseline covariates. Cox proportional hazards regression models, conditioned on propensity score-matched pairs, were used to estimate hazard ratios (HRs) of DKA for new users of SGLT2i versus other AHAs. When I <40%, a combined HR across the four databases was estimated.
Using the broad definition of T2DM, new users of SGLT2i had an increased risk of DKA versus sulfonylureas (HR [95% CI]: 1.53 [1.31-1.79]), DPP-4i (1.28 [1.11-1.47]), GLP-1 receptor agonists (1.34 [1.12-1.60]), metformin (1.31 [1.11-1.54]), and insulinotropic AHAs (1.38 [1.15-1.66]). Using the narrow definition of T2DM, new users of SGLT2i had an increased risk of DKA versus sulfonylureas (1.43 [1.01-2.01]). New users of SGLT2i had a lower risk of DKA versus insulin and a similar risk as thiazolidinediones, regardless of T2DM definition.
Increased risk of DKA was observed for new users of SGLT2i versus several non-SGLT2i AHAs when T2DM was defined broadly. When T2DM was defined narrowly to exclude possible misclassified patients, an increased risk of DKA with SGLT2i was observed compared with sulfonylureas.
比较新使用钠-葡萄糖协同转运蛋白 2 抑制剂(SGLT2i)与其他类别的抗高血糖药物(AHA)的 2 型糖尿病(T2DM)患者中糖尿病酮症酸中毒(DKA)的发生率。
利用四项美国大型理赔数据库,采用广泛(所有 T2DM 患者)和狭义(旨在排除 1 型糖尿病或被错误归类为 T2DM 的继发性糖尿病患者)的 T2DM 定义来确定新使用 SGLT2i 的患者。通过暴露倾向评分对 SGLT2i 新使用者和七种对照组 AHA 进行(1:1)匹配,以调整基线协变量的不平衡。使用条件于倾向评分匹配对的 Cox 比例风险回归模型来估计 SGLT2i 新使用者与其他 AHA 相比 DKA 的危险比(HR)。当 I <40%时,对四个数据库进行综合 HR 估计。
使用广泛的 T2DM 定义,与磺酰脲类药物(HR[95%CI]:1.53[1.31-1.79])、DPP-4i(1.28[1.11-1.47])、GLP-1 受体激动剂(1.34[1.12-1.60])、二甲双胍(1.31[1.11-1.54])和胰岛素增敏 AHA(1.38[1.15-1.66])相比,新使用 SGLT2i 的患者 DKA 风险增加。使用狭义的 T2DM 定义,与磺酰脲类药物相比,新使用 SGLT2i 的患者 DKA 风险增加(1.43[1.01-2.01])。无论 T2DM 定义如何,新使用 SGLT2i 的患者 DKA 风险低于胰岛素,风险与噻唑烷二酮相似。
当 T2DM 被广泛定义时,与几种非 SGLT2i AHA 相比,新使用 SGLT2i 的患者 DKA 风险增加。当 T2DM 被狭义定义以排除可能的错误分类患者时,与磺酰脲类药物相比,新使用 SGLT2i 的患者 DKA 风险增加。