Jodoin Marianne, Rouleau Dominique M, Therrien Erik, Chauny Jean-Marc, Sandman Emilie, Larson-Dupuis Camille, Leduc Stephane, Gosselin Nadia, De Beaumont Louis
Centre de Recherche de l'Hôpital Sacré-Coeur de Montréal, Montréal, Québec, Canada.
Départment de Psychologie, Université de Montréal, Montréal, Québec, Canada.
Bone Rep. 2019 Aug 13;11:100222. doi: 10.1016/j.bonr.2019.100222. eCollection 2019 Dec.
This study seeks to evaluate the incidence rate of heterotopic ossification (HO) formation in patients afflicted by an isolated limb fracture (ILF) and a concomitant mild traumatic brain injury (mTBI).
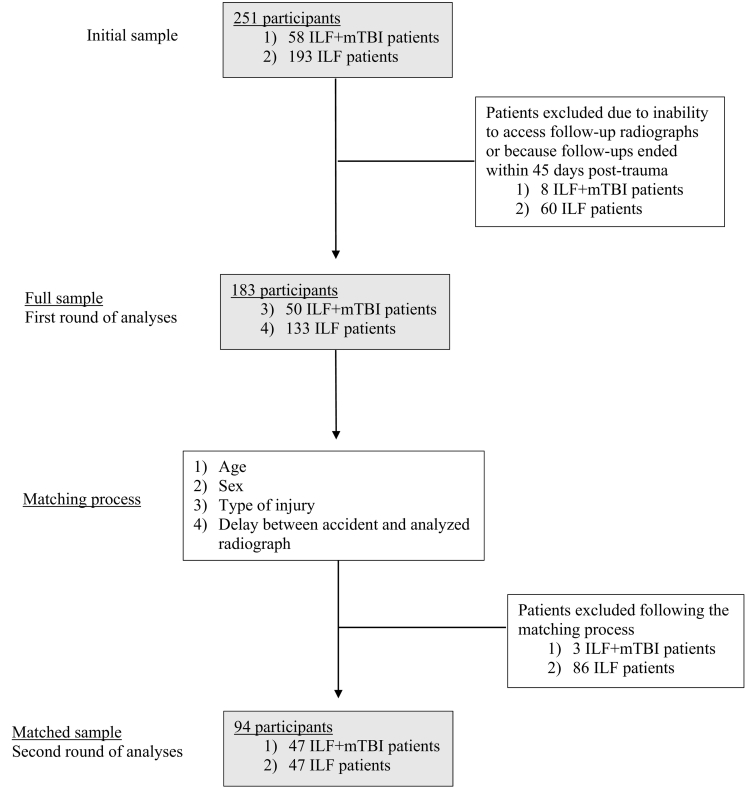
The current study is an observational study including ILF patients with or without a concomitant mTBI recruited from an orthopedic clinic of a Level 1 Trauma Hospital. Patients were diagnosed with a mTBI according to the American Congress of Rehabilitation Medicine (ACRM) criteria. Radiographs taken on average 3 months post-trauma were analyzed separately by two distinct specialists for the presence of HO proximally to the fracture site (joints or extra joints). Both raters referred to Brooker's and Della's Valle's classification to establish signs of HO. First, analyses were conducted for the full sample. Secondly, a matched cohort was used in order to control for specific factors, namely age, sex, type of injury, and time elapsed between the accident and the analyzed radiograph.
The full sample included a total of 183 patients with an ILF (94 females; 47.5 years old), of which 50 had a concomitant mTBI and 133 without. Radiographic evidence of HO was significantly higher in patients with an ILF and a mTBI compared to ILF patients (X = 6.50; = 0.01). The matched cohort consisted of 94 participants (i.e.; 47 patients from the ILF + mTBI group and 47 patients from the ILF group). Again, ILF + mTBI patients presented significantly higher rates of HO signs in comparison to ILF patients (X = 3.69; = 0.04). Presence of HO was associated with prolonged delays to return to work (RTW) only in ILF + mTBI patients (F = 4.055; = 0.05) but not in ILF patients (F = 0.823; = 0.37).
Study findings suggest that rates of HO are significantly higher proximally to fracture sites when ILF patients sustain a concomitant mTBI, even after controlling for factors known to influence HO. Moreover, results show that HO is associated with a prolonged RTW only in ILF patients with a concomitant mTBI but not in ILF-only patients. The impact of mTBI on HO formation warrants further attention to detect early signs of HO, to identify shared physiopathological mechanisms and, ultimately, to design targeted therapies.
本研究旨在评估孤立性肢体骨折(ILF)合并轻度创伤性脑损伤(mTBI)患者异位骨化(HO)形成的发生率。
本研究为一项观察性研究,纳入了从一级创伤医院骨科诊所招募的有或无合并mTBI的ILF患者。根据美国康复医学大会(ACRM)标准诊断患者是否患有mTBI。由两位不同的专家分别分析创伤后平均3个月拍摄的X线片,以检查骨折部位近端(关节或关节外)是否存在HO。两位评估者均参考布鲁克(Brooker)和德拉·瓦莱(Della's Valle)的分类标准来确定HO的体征。首先,对整个样本进行分析。其次,为控制特定因素,即年龄、性别、损伤类型以及事故与所分析X线片之间的时间间隔,使用了匹配队列。
整个样本共包括183例ILF患者(94例女性;平均年龄47.5岁),其中50例合并mTBI,133例未合并。与单纯ILF患者相比,ILF合并mTBI患者的HO影像学证据明显更高(X = 6.50;P = 0.01)。匹配队列由94名参与者组成(即47例来自ILF + mTBI组,47例来自ILF组)。同样,与ILF患者相比,ILF + mTBI患者的HO体征发生率明显更高(X = 3.69;P = 0.04)。仅在ILF + mTBI患者中,HO的存在与恢复工作(RTW)的延迟延长相关(F = 4.055;P = 0.05),而在ILF患者中则无此关联(F = 0.823;P = 0.37)。
研究结果表明,即使在控制了已知影响HO的因素后,ILF合并mTBI患者骨折部位近端的HO发生率仍显著更高。此外,结果显示,仅在合并mTBI的ILF患者中HO与RTW延迟延长相关,而在单纯ILF患者中则不然。mTBI对HO形成的影响值得进一步关注,以检测HO的早期体征,确定共同的生理病理机制,并最终设计针对性的治疗方法。