Department of Trauma Surgery, University Medical Center Utrecht, Suite: G04.228, Heidelberglaan 100, 3584 CX, Utrecht, The Netherlands.
Department of Trauma Surgery, Harborview Medical Center, Seattle, USA.
Eur J Trauma Emerg Surg. 2021 Feb;47(1):137-143. doi: 10.1007/s00068-019-01208-z. Epub 2019 Aug 30.
Venous thromboembolisms (VTE) are a major concern after acute survival from trauma. Variations in treatment protocols for trauma patients exist worldwide. This study analyzes the differences in the number of VTE events and the associated complications of thromboprophylaxis between two level I trauma populations utilizing varying treatment protocols.
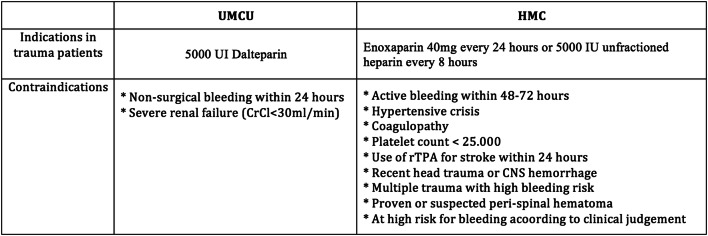
International multicenter trauma registry-based study was performed at the University Medical Center Utrecht (UMCU) in The Netherlands (early commencement chemical prophylaxis), and Harborview Medical Center (HMC) in the United States (restrictive early chemical prophylaxis). All severely injured patients (ISS ≥ 16), aged ≥ 18 years, and admitted in 2013 were included. Primary outcomes were VTE [deep venous thrombosis (DVT) (no screening), pulmonary embolism (PE)], and hemorrhagic complications.
In UMCU, 279 patients were included and in HMC, 974 patients. Overall, 75% of the admitted trauma patients in UMCU and 81% in HMC (p < 0.001) received thromboprophylaxis, of which 100% in and 75% at, respectively, UMCU and HMC consisted of chemical prophylaxis. From these patients, 72% at UMCU and 47% at HMC (p < 0.001) were treated within 48 h after arrival. At UMCU, 4 patients (1.4%) (PE = 3, DVT = 1) and HMC 37 patients (3.8%) (PE = 22, DVT = 16; p = 0.06) developed a VTE. At UMCU, a greater percent of patients with VTE had traumatic brain injuries (TBI). Most VTE occurred despite adequate prophylaxis being given (75% UMCU and 81% HMC). Hemorrhagic complications occurred in, respectively, 4 (1.4%) and 10 (1%) patients in UMCU and HMC (p = 0.570). After adjustment for age, ISS, HLOS, and injury type, no significant difference was demonstrated in UMCU compared to HMC for the development of VTE, OR 2.397, p = 0.102 and hemorrhagic complications, OR 0. 586, p = 0.383.
A more early commencement protocol resulted in almost twice as much chemical prophylaxis being started within the first 48 h in comparison with a more delayed initiation of treatment. Interestingly, most episodes of VTE developed while receiving recommended prophylaxis. Early chemical thromboprophylaxis did not significantly increase the bleeding complications and it appears to be safe to start early.
创伤后急性存活的患者存在静脉血栓栓塞(VTE)的重大隐患。全世界对创伤患者的治疗方案存在差异。本研究分析了使用不同治疗方案的两个一级创伤人群中,VTE 事件数量和血栓预防相关并发症的差异。
在荷兰乌得勒支大学医学中心(UMCU)(早期开始化学预防)和美国 Harborview 医疗中心(HMC)(限制早期化学预防)进行了基于国际多中心创伤登记处的研究。纳入所有严重受伤患者(ISS≥16 岁),年龄≥18 岁,于 2013 年入院。主要结局为 VTE[深静脉血栓形成(DVT)(无筛查),肺栓塞(PE)]和出血性并发症。
UMCU 纳入 279 例患者,HMC 纳入 974 例患者。总体而言,UMCU 入院创伤患者中有 75%,HMC 中有 81%(p<0.001)接受了血栓预防,其中 UMCU 和 HMC 分别有 100%和 75%的患者接受了化学预防。在这些患者中,UMCU 有 72%,HMC 有 47%(p<0.001)在到达后 48 小时内接受治疗。UMCU 有 4 例(1.4%)(PE=3,DVT=1)和 HMC 有 37 例(3.8%)(PE=22,DVT=16;p=0.06)发生 VTE。在 UMCU,发生 VTE 的患者中,创伤性脑损伤(TBI)的比例更高。尽管给予了充分的预防措施,但大多数 VTE 仍发生(UMCU 为 75%,HMC 为 81%)。在 UMCU 和 HMC,分别有 4 例(1.4%)和 10 例(1%)患者发生出血性并发症(p=0.570)。在调整年龄、ISS、HLOS 和损伤类型后,与 HMC 相比,UMCU 发生 VTE 的风险无显著差异,OR 2.397,p=0.102,出血性并发症的风险也无显著差异,OR 0.586,p=0.383。
与治疗开始延迟相比,早期开始方案可使前 48 小时内开始化学预防的比例增加近两倍。有趣的是,大多数 VTE 发生在接受推荐预防措施的同时。早期化学血栓预防并未显著增加出血并发症,且早期开始似乎是安全的。