Division of Hematology, Department of Medicine, University of Ottawa and Ottawa Hospital Research Institute, Ottawa, Canada.
Center for International Blood and Marrow Transplant Research, Medical College of Wisconsin, Milwaukee, Wisconsin; Division of Hematology/Oncology, Department of Medicine, Medical College of Wisconsin, Milwaukee, Wisconsin.
Biol Blood Marrow Transplant. 2019 Dec;25(12):2398-2407. doi: 10.1016/j.bbmt.2019.08.012. Epub 2019 Aug 29.
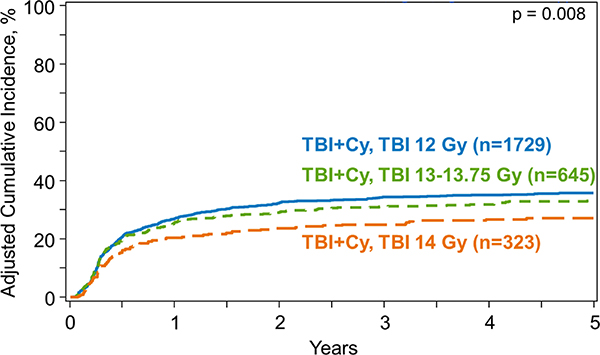
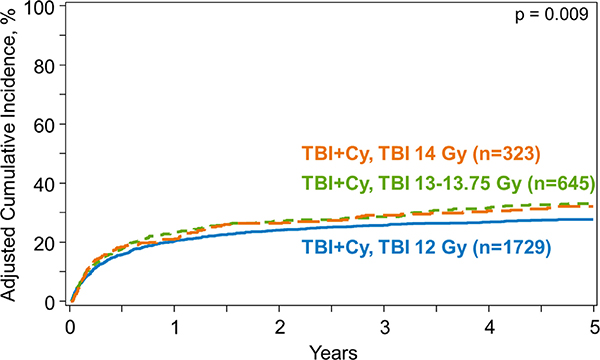
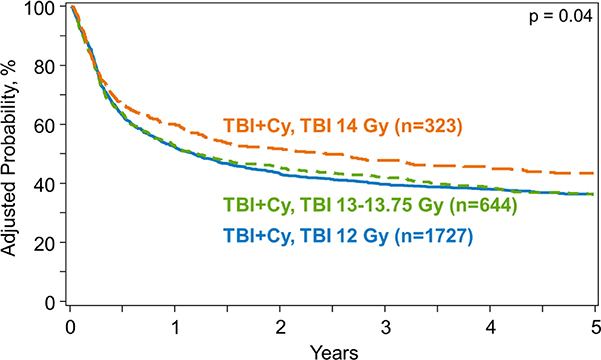
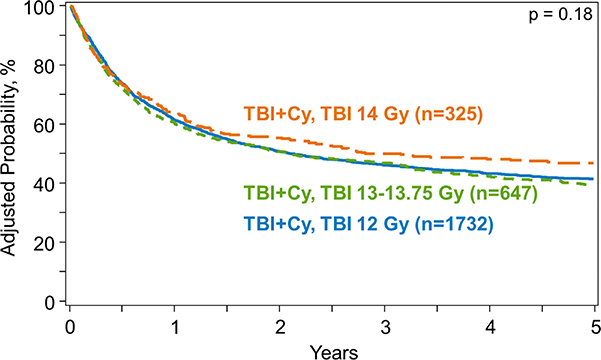
Malignancy relapse is the most common cause of treatment failure among recipients of hematopoietic cell transplantation (HCT). Conditioning dose intensity can reduce disease relapse but is offset by toxicities. Improvements in radiotherapy techniques and supportive care may translate to better outcomes with higher irradiation doses in the modern era. This study compares outcomes of recipients of increasing doses of high-dose total body irradiation (TBI) divided into intermediate high dose (IH; 13-13.75 Gy) and high dose (HD; 14 Gy) with standard dose (SD; 12 Gy) with cyclophosphamide. A total of 2721 patients ages 18 to 60 years with hematologic malignancies receiving HCT from 2001 to 2013 were included. Cumulative incidences of nonrelapse mortality (NRM) at 5 years were 28% (95% confidence interval [CI], 25% to 30%), 32% (95% CI, 29% to 36%), and 34% (95% CI, 28% to 39%) for SD, IH, and HD, respectively (P = .02). Patients receiving IH-TBI had a 25% higher risk of NRM compared with those receiving SD-TBI (12 Gy) (P = .007). Corresponding cumulative incidences of relapse were 36% (95% CI, 34% to 38%), 32% (95% CI, 29% to 36%), and 26% (95% CI, 21% to 31%; P = .001). Hazard ratios for mortality compared with SD were 1.06 (95% CI, .94 to 1.19; P = .36) for IH and .89 (95% CI, .76 to 1.05; P = .17) for HD. The study demonstrates that despite improvements in supportive care, myeloablative conditioning using higher doses of TBI (with cyclophosphamide) leads to worse NRM and offers no survival benefit over SD, despite reducing disease relapse.
恶性肿瘤复发是造血细胞移植(HCT)受者治疗失败的最常见原因。预处理剂量强度可以降低疾病复发率,但会被毒性所抵消。放射治疗技术和支持性护理的改进可能会使现代接受更高剂量照射的患者获得更好的结果。本研究比较了接受递增剂量高剂量全身照射(TBI)的患者的结局,这些患者分为中高剂量(IH;13-13.75Gy)和高剂量(HD;14Gy)与标准剂量(SD;12Gy)与环磷酰胺联合。共纳入 2721 例年龄在 18 至 60 岁之间的血液系统恶性肿瘤患者,他们在 2001 年至 2013 年期间接受了 HCT。5 年非复发死亡率(NRM)的累积发生率分别为 28%(95%置信区间[CI],25%至 30%)、32%(95%CI,29%至 36%)和 34%(95%CI,28%至 39%),分别为 SD、IH 和 HD(P=0.02)。接受 IH-TBI 的患者与接受 SD-TBI(12Gy)的患者相比,NRM 的风险增加了 25%(P=0.007)。相应的累积复发率分别为 36%(95%CI,34%至 38%)、32%(95%CI,29%至 36%)和 26%(95%CI,21%至 31%;P=0.001)。与 SD 相比,死亡率的风险比分别为 IH 为 1.06(95%CI,0.94 至 1.19;P=0.36)和 HD 为 0.89(95%CI,0.76 至 1.05;P=0.17)。该研究表明,尽管支持性护理有所改善,但使用更高剂量 TBI(与环磷酰胺联合)进行清髓性预处理会导致更差的 NRM,并且尽管降低了疾病复发率,但并不能提供生存获益。