Yonsei University Health System Seoul Republic of Korea.
Division of Cardiology CHA University Seongnam Republic of Korea.
J Am Heart Assoc. 2019 Sep 3;8(17):e013204. doi: 10.1161/JAHA.119.013204. Epub 2019 Aug 31.
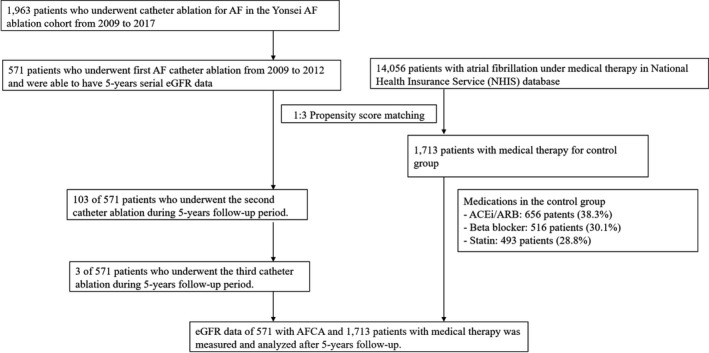
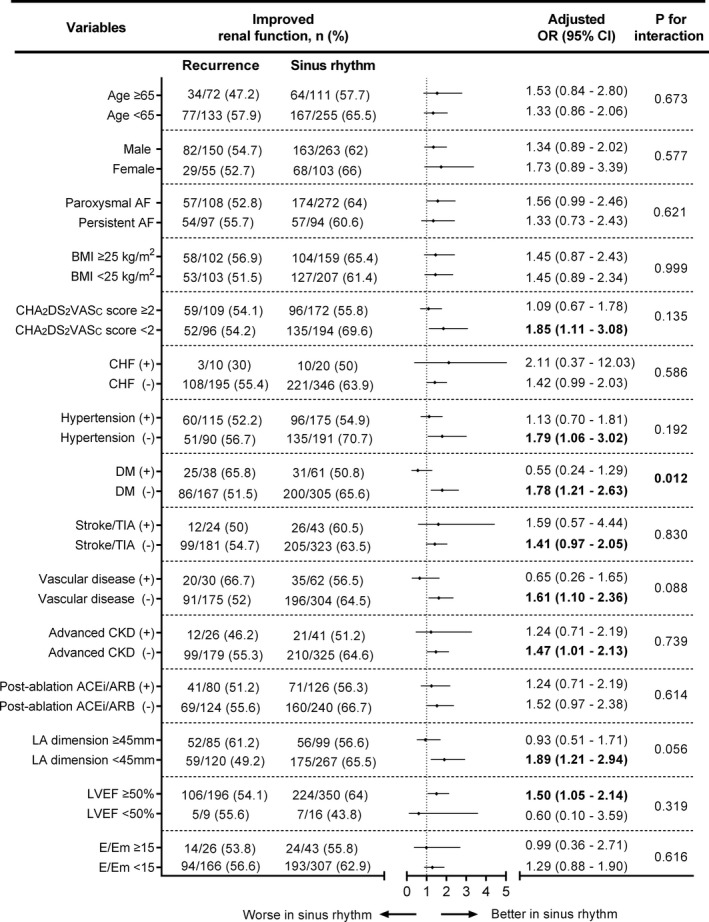
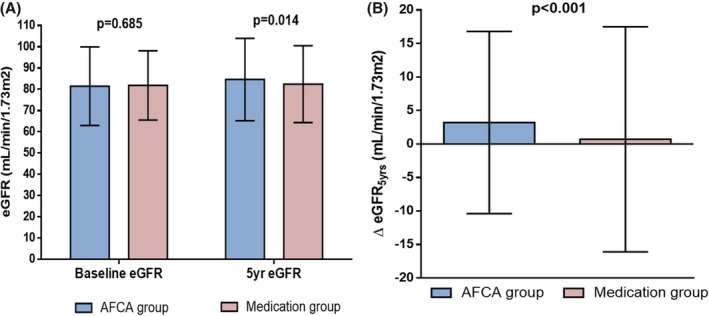
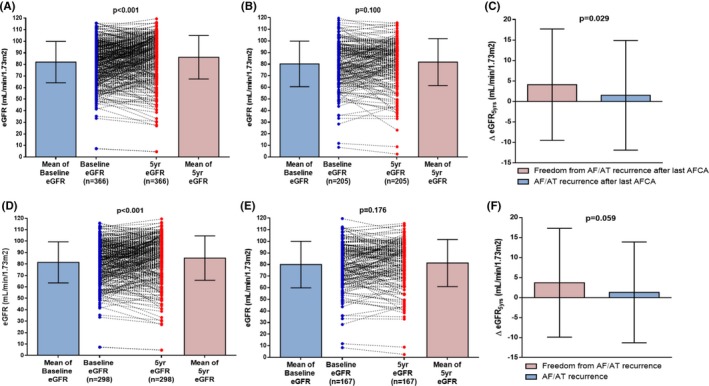
Background Although it has been reported that renal function can improve after catheter ablation of atrial fibrillation (AF), long-term changes in renal function and its relationship to rhythm outcomes have not yet been evaluated. We explored the 5-year change in estimated glomerular filtration rate (eGFR) in AF patients depending on medical therapy and catheter ablation. Methods and Results Among 1963 patients who underwent AF catheter ablation and 14 056 with AF under medical therapy in the National Health Insurance Service database, we compared 571 with AF catheter ablation (59±10 years old, 72.3% male, and 66.5% paroxysmal AF) and 1713 with medical therapy after 1:3 propensity-score matching. All participants had 5 years of serial eGFR data (Chronic Kidney Disease-Epidemiology Collaboration [CKD-EPI] method). Catheter ablation improved eGFR (P<0.001), but medical therapy did not. In 2284 matched patients, age (adjusted odds ratio [OR], 0.98 [0.97-0.99]; P<0.001) and AF catheter ablation (adjusted OR, 2.02 [1.67-2.46]; P<0.001) were independently associated with an improved eGFR. Among 571 patients who underwent AF ablation, freedom from AF/atrial tachycardia recurrence after the last AF ablation procedure was independently associated with an improved eGFR (adjusted OR, 1.44 [1.01-2.04]; P=0.043), especially in patients without diabetes mellitus (adjusted OR, 1.78 [1.21-2.63]; P=0.003, P for interaction=0.012). Although underlying renal dysfunction (<60 mL/min/1.73m) was associated with atrial structural remodeling (adjusted OR, 1.05 [1.00-1.11]; P=0.046), it did not affect the AF ablation rhythm outcome. Conclusions AF catheter ablation significantly improved renal function over a 5-year follow-up, especially in patients maintaining sinus rhythm without preexisting diabetes mellitus.
虽然已有研究报道,房颤(AF)导管消融后肾功能可以改善,但长期肾功能变化及其与节律转归的关系尚未得到评估。我们探讨了 AF 患者在接受药物治疗和导管消融治疗后肾小球滤过率(eGFR)的 5 年变化。
在国家健康保险服务数据库中,我们比较了 1963 例接受 AF 导管消融和 14056 例接受药物治疗的 AF 患者,其中 571 例接受了 AF 导管消融(59±10 岁,72.3%为男性,66.5%为阵发性 AF),1713 例接受了药物治疗,采用 1:3 倾向评分匹配。所有参与者均有 5 年的连续 eGFR 数据(慢性肾脏病流行病学合作研究[CKD-EPI]方法)。导管消融可改善 eGFR(P<0.001),但药物治疗无效。在 2284 例匹配患者中,年龄(校正优势比[OR],0.98[0.97-0.99];P<0.001)和 AF 导管消融(校正 OR,2.02[1.67-2.46];P<0.001)与 eGFR 改善独立相关。在 571 例接受 AF 消融的患者中,最后一次 AF 消融后无 AF/房性心动过速复发与 eGFR 改善独立相关(校正 OR,1.44[1.01-2.04];P=0.043),尤其是在无糖尿病的患者中(校正 OR,1.78[1.21-2.63];P=0.003,P 交互=0.012)。虽然基础肾功能不全(<60 mL/min/1.73 m)与心房结构重塑相关(校正 OR,1.05[1.00-1.11];P=0.046),但它并不影响 AF 消融的节律转归。
AF 导管消融可显著改善肾功能,5 年随访期间尤其在无糖尿病且维持窦性心律的患者中。